
Considerations for egg freezing: a practical guide
Some additional notes on practical steps towards egg freezing


This month, I underwent egg freezing at IVI Valencia in Spain. The procedure went smoothly and I experienced minimal side effects. In total, 11 mature eggs were collected — a result that aligns well with the average for my age.
While the quality expected of eggs retrieved at my age means the chances of achieving a live birth from these eggs is quite high, I want to give myself the greatest possible certainty. With that in mind, I plan to do a second round, with the aim of reaching at least 20 eggs in total.
The timing of my freezing is quite good, because in the coming days, an article I co-authored with Luzia Bruckamp for Works in Progress is coming out in the next few days. There, we demistify the entire process, showing that egg freezing works when done at the right age and at the right clinic, explaining the underpinnings of female fertility decline with age and giving some advice on the steps to start the process. It’s in many ways a follow-up on my earlier article with them, Fertility on Demand, where I make the case that one way to allow women to pursue the careers they want is through the aid of reproductive technologies.
The main article, however, doesn't cover every practical detail of the process in depth. This piece contains some of these details.
Practical considerations
The most important considerations are cost; the optimal time to freeze one’s eggs; choosing a clinic; the choice between freezing eggs or embryos, as well as considering the influence of any reproductive conditions.
Costs
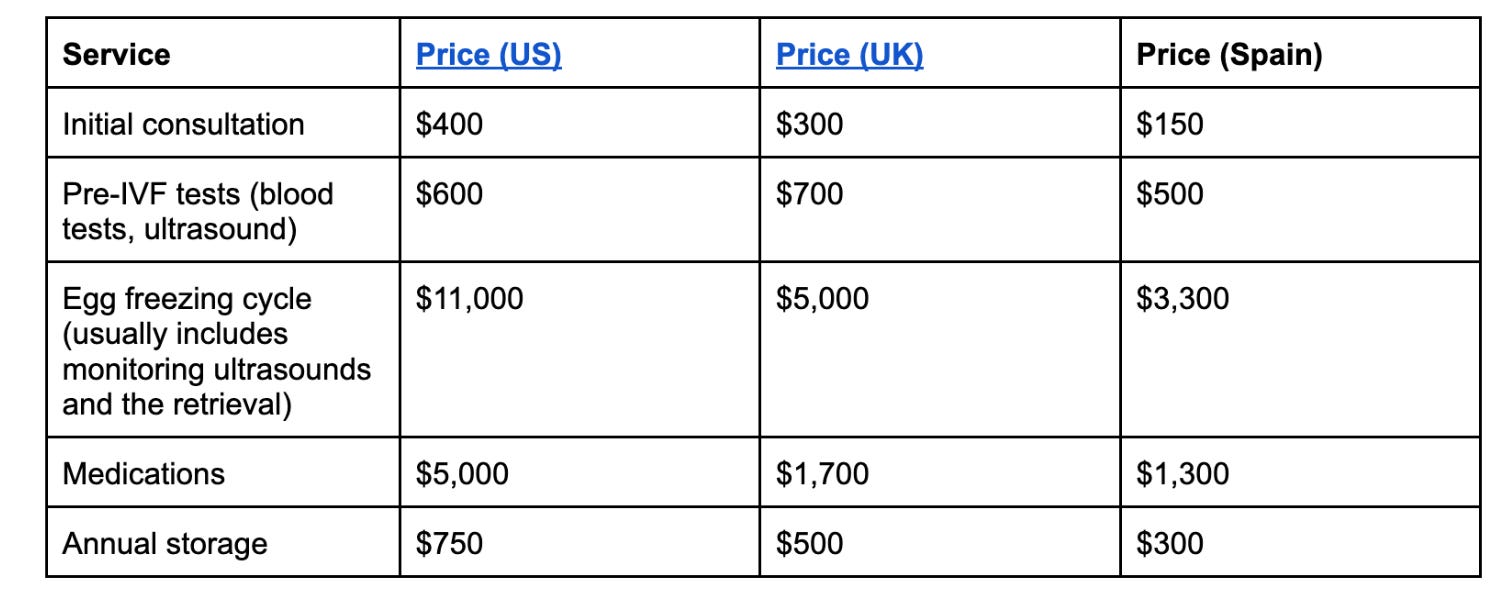
Table 1. Average costs of the egg freezing procedure across three different countries. There might be additional optional costs for add-ons like PGT-A. Note that there is also substantial variation between clinics, especially in the US.
To avoid unexpected costs, we advise inquiring about all prices with the clinic you are choosing. It is particularly common for the cost of medications, those of additional tests like ultrasounds and blood tests, or annual storage to be excluded from the total. Clinics also often offer discounts for purchasing multiple cycles upfront so you might want to plan to do two cycles depending on your expected number of eggs per cycle.
Egg freezing is expensive in the US. In total, an egg freezing cycle including tests and medications will cost around $17,000. The UK is more affordable, at roughly $8,000 per cycle and Spain is even better, averaging $5,000. Luckily, many international clinics offer the option to conduct consultations online and travel only for the final retrieval procedure to the clinic. But bear in mind that they might need more than one cycle to get enough eggs.
If you’re not able to pay this out-of-pocket, some companies offer egg freezing as part of their insurance policies. Another alternative is to sell off half your eggs through services like Cofertility and Freeze and Share, which covers the cost of the procedure.
The optimal time to egg freeze
If cost is not a constraint, the optimal age for egg freezing is around 25 to 27, when a single cycle is more likely to yield enough eggs and a greater proportion of those eggs are euploid.
That said, egg freezing is a significant financial undertaking, and for many women that reality cannot be set aside. Since most women can still conceive naturally even in their late thirties, it may make sense to wait a little longer and factor in personal circumstances — relationship status, whether and when children feel like a realistic prospect, and so on.
Weighing all of this together, somewhere between 29 and 32 seems like a reasonable sweet spot. Official guidance typically cites anything under 35 as acceptable, but this reflects the older assumption that fertility drops sharply at that age. The evidence now suggests meaningful egg quality decline begins well before 35 — so from the standpoint of egg freezing specifically, doing so before 32 is likely the better course.
One useful data point when weighing up the timing is your antral follicle count (AFC), which can be measured via ultrasound without committing to a full cycle. As discussed in the main article, the number of eggs retrieved in a cycle tends to be roughly 80% of your AFC, making it a meaningful predictor of outcomes. If your AFC is low for your age, that is a strong signal to act sooner rather than later — and possibly to plan for more than one cycle from the outset.
Alternatively, you might measure your anti-mullerian hormone, or AMH, through a blood test. While not as precise as a follicle count for predicting the outcome of a single cycle, it can be a useful warning for low ovarian reserve. If you are in the slightly low or low categories, you might start freezing sooner rather than later.
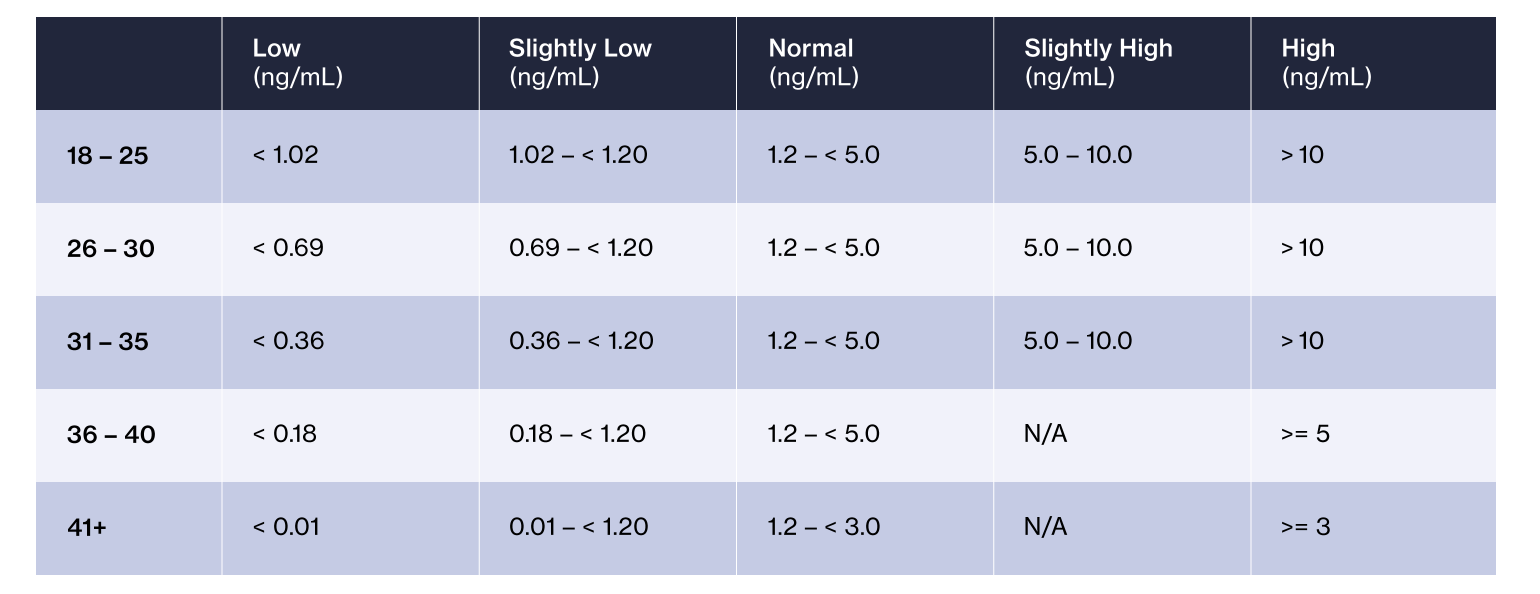
Table 2. Egg reserve and AMH levels. From here.
Choosing the right clinic
Not all IVF clinics are created equal. While you might worry that comparing success rates between clinics is tricky due to selection bias, in practice it seems like they actually provide a good sense of clinic quality. Firstly, some of the best clinics accept difficult cases more often, but are so much better that they still achieve higher success rates. Secondly, IVF patients are a relatively homogeneous group with high socio-economic status.
We can also tell that technical quality varies widely among clinics. For example, low oxygen levels are important in embryo culture because early embryos are not adapted to the high oxygen concentration found in room air. In vivo, mammalian embryos develop in the fallopian tube and uterus at oxygen concentrations around two to eight percent, far lower than the 21 percent oxygen of atmospheric air. Yet many clinics still fail to use natural oxygen levels in their embryo culture chambers.
Overall, the difference in success rates between clinics should give you important information about the clinic’s quality, as long as you subset for your age group. It is generally advisable to double check the numbers you see on clinics’ websites against official statistics. The most comprehensive reports can be found in the US, through the CDC website. There are also websites that provide rankings of fertility clinics through an evaluation process that included a nationwide online survey of reproductive endocrinologists, infertility specialists, obstetricians and gynecologists. In the UK, the UK’s fertility regulator provides a Choose your clinic tool where you can see success rates for each clinic compared to the national average. In Spain, the equivalent is Reproduccion Asistida ORG.
What should I look for?
There are three important metrics: success per embryo transfer, success per IVF cycle and the frozen egg survival rate. Unfortunately, no official agency records frozen egg survival and only the CDC reports both success per embryo transfer and success per IVF cycle.
Success per embryo transfer measures the live birth rate once a viable embryo has been transferred into the uterus. It’s an indicator of the clinic’s skill at the final step of the process. Success per cycle, on the other hand, is a more comprehensive metric that measures the live birth rate from the start of an egg retrieval cycle. This includes all the attrition points along the way, such as egg retrieval, fertilization, and embryo development.
Success per embryo transfer is a useful metric because different women have different ovarian reserves which is independent of clinic. But it does not capture how good a clinic is at the steps before embryo transfer, including the key bottleneck of turning eggs into embryos, and it can be easily influenced by what the clinic considers to be a transferable embryo. If only very high quality embryos are considered for transfer, then the success per embryo transferred can be high, but the woman might overall have fewer embryos available.
This brings us to the question of how clinics choose what a high quality embryo is. The most objective test is for aneuploidy, whether the embryo has the right number of chromosomes. Most clinics also check whether an embryo is morphologically normal, meaning that its visible physical characteristics align with established developmental benchmarks.
Euploid embryos have a roughly 65 percent chance of resulting in a live birth. Preimplantation tests for aneuploidy, which are more common in the US than in the UK, will therefore push up the success rate when measured per embryo transfer, since a clinic using them will implant only euploid embryos..
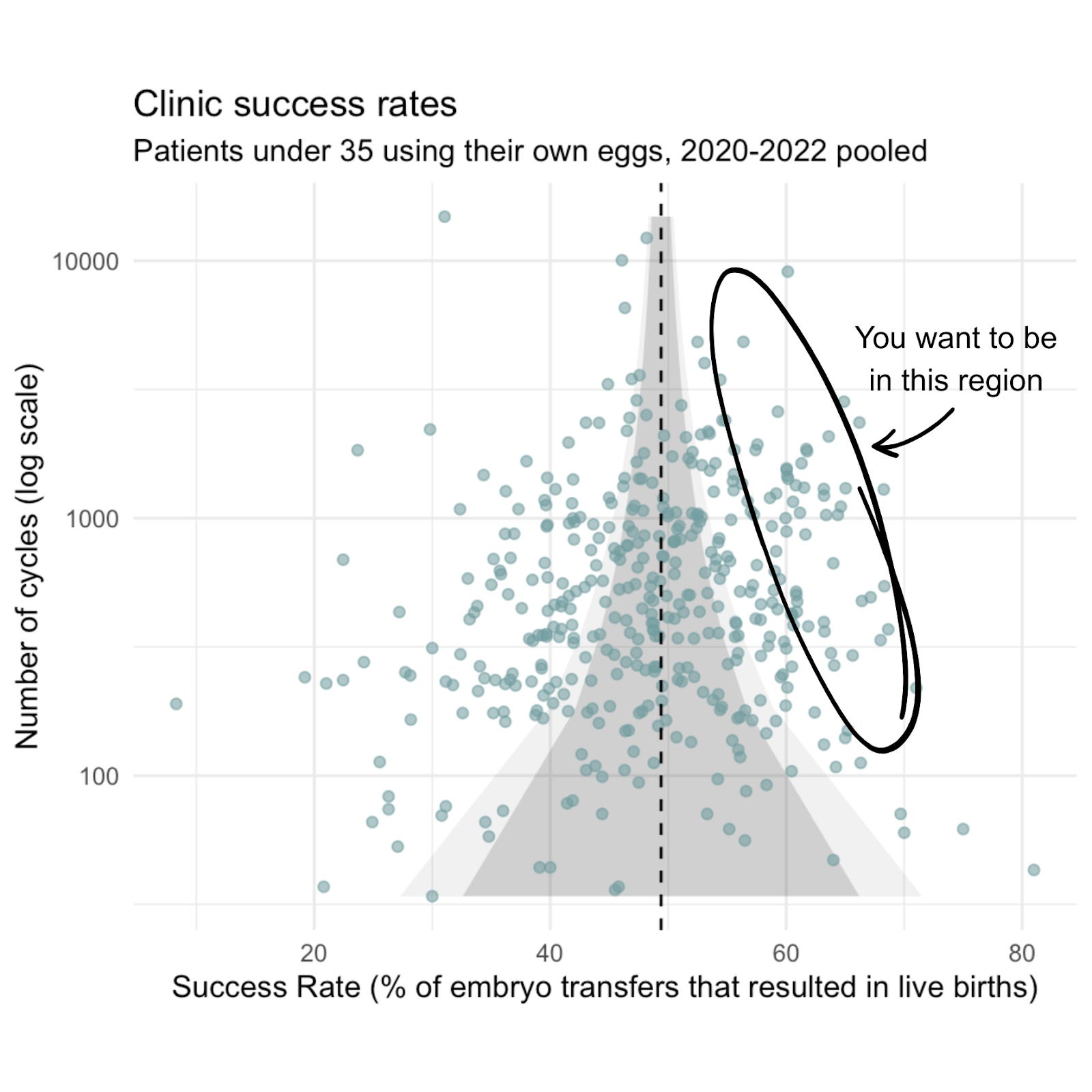
Figure 1. Clinic success rates for patients under 35 using their own eggs (2020–2022 from US fertility clinics pooled). Each point represents a U.S. fertility clinic, showing the relationship between the number of IVF cycles performed (log scale) and success rate (percentage of embryo transfers resulting in live births). The lighter (darker) shaded area indicates where we would expect clinics to fall 99% (95%) of the time if the clinic had a “true” underlying success rate of 49%, the average across all cycles The circled region marks the high-performing clinics with both high success rates and substantial cycle volumes.
Source: NASS data provided by the CDC for 2020, 2021, and 2022, own analysis
What about egg survival?
Unfortunately, clinics do not have to report the success of egg freezing itself (how many eggs survive the freezing and thawing process) to central regulators.
Some clinics have peer-reviewed studies that include egg survival post thawing: for example, NYU Langone in US (79 percent survival rate), IVI Valencia (85 percent survival rate) in Spain and Guy’s & St Thomas’ NHS (UK) (74 percent survival rate). Already from these studies we can see variability. However, these are older studies, carried out around the time when vitrification was first being introduced. Furthermore, the women in these studies have a median age of 36-38 and survival of older eggs tends to be lower post freezing and thawing.
The European Society of Human Reproduction and Embryology now believes that 95 to 100 percent of eggs from donors under 35 years old should survive, and labs have long been able to reach this rate when using donor eggs. IVI Valencia reported a 96.7 percent survival rate for donor eggs in 2007. Since clinics pay for eggs from donors, they have an even stronger incentive than usual to maximize the success of vitrification and warming, and so may have optimized these processes. You may wish to use a clinic that also does egg donation.
Freezing eggs versus embryos
If you are in a stable relationship or decided upon the father of your child(ren), consider freezing embryos, as they have slightly higher survival rates post-thaw (95 versus 90 percent). Another advantage is lower variability between clinics and between women. You also reduce the amount of uncertainty once you know how many embryos you have: Although failures are always possible, fewer than five percent of women cannot achieve pregnancy after implanting three euploid embryos.
Endometriosis
Endometriosis is a chronic, very poorly understood disease characterized by the growth of endometrial (uterus-lining-like) tissue outside the uterus, affecting an estimated seven to ten percent of reproductive-aged women. Adenomyosis describes the condition when the endometrial tissue is in the uterine wall.
Endometriosis and adenomyosis have been associated with reduced ovarian reserve and lower egg quality. Given that both endometriosis and adenomyosis can worsen with time, freezing eggs at a young age could be an important pre-emptive measure to counteract an accelerated decline of egg quality with age.
However, women with adenomyosis should be careful about delaying pregnancy because adenomyosis worsens implantation rates independently of egg quality. A retrospective study conducted between 2016 and 2022 on 456 patients shows that the live birth rate after euploid embryo transfer was 25 percent in patients with adenomyosis compared to 47 percent in controls. (The latest studies using donor eggs, which allow for studying live birth rates while controlling for confounders like ovarian response, suggest that the same is not the case for endometriosis.) Considering the above evidence that adenomyosis can progress with age, egg freezing may not provide good insurance against infertility.
Polycystic ovary syndrome
Polycystic ovary syndrome is one of the most common endocrine disorders, affecting approximately 15 percent of women of reproductive age. It is characterized by irregular ovulation or anovulation (no ovulation), hyperandrogenism (higher male hormones), and polycystic ovarian morphology (this refers to arrested follicles visible on an ultrasound). Women with PCOS typically have a higher antral follicle count (AFC) and often produce a larger number of oocytes during stimulation cycles. This makes egg banking more efficient. On the other hand, the risk of ovarian hyperstimulation for women with PCOS is higher. here are also other important caveats: Although egg quantity is typically high, several studies have shown that women with PCOS that have a hyperandrogenic phenotype can experience more pregnancy complications. Optimizing metabolic health prior to implantation, through lifestyle interventions or, in some cases, medications such as metformin, can help.
Distribution of number of eggs collected and fertilized
We also had some fascinating plots that didn’t make it into the final article, drawing on data from the HFEA, the UK’s fertility regulator. These cover the distribution of eggs retrieved per woman across a single cycle, as well as the downstream distributions of fertilised eggs and euploid embryos.
The euploid embryo distribution is particularly striking. As a rough guide, 2 euploid embryos translates to around an 80% chance of a live birth, and 3 is close to a guarantee — only around 5% of women with 3 euploid embryos see no pregnancy after transfer. Among those for whom cycles fail, implantation issues are the likely culprit. Taken together, the data suggest that for most women between 18 and 34, a single cycle is enough to make a live birth achievable.
These distributions are also worth keeping in mind in the context of embryo selection services, such as those offered by Herasight, which are growing in popularity. The more embryos available, the more powerful these tools become, so having a realistic sense of what a single cycle is likely to yield is genuinely useful when deciding how to proceed.
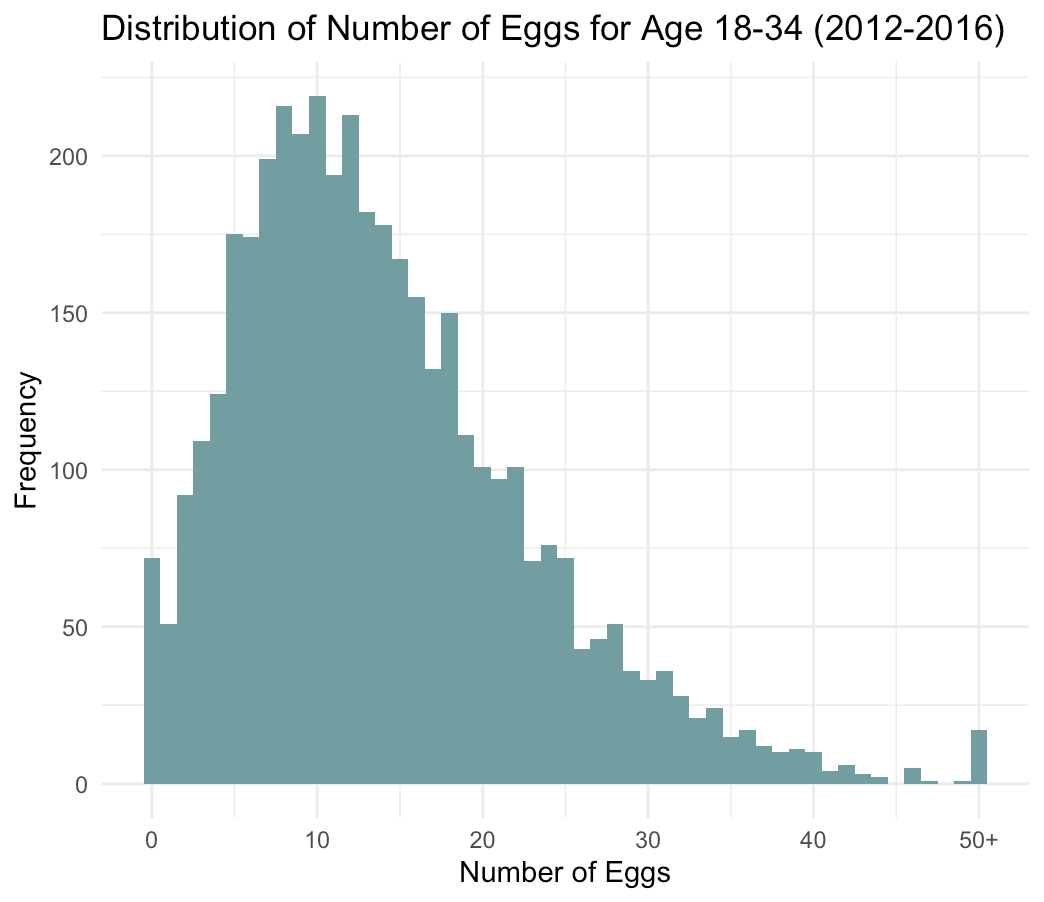
Figure 2. Distribution of the number of eggs collected for women between 18 and 34 undergoing egg or embryo freezing across clinics in the UK. There is considerable variation between women in the number of eggs collected in an egg or embryo freezing cycle. Source: HFEA register data, 2012-2016, Luzia Bruckamp’s analysis.
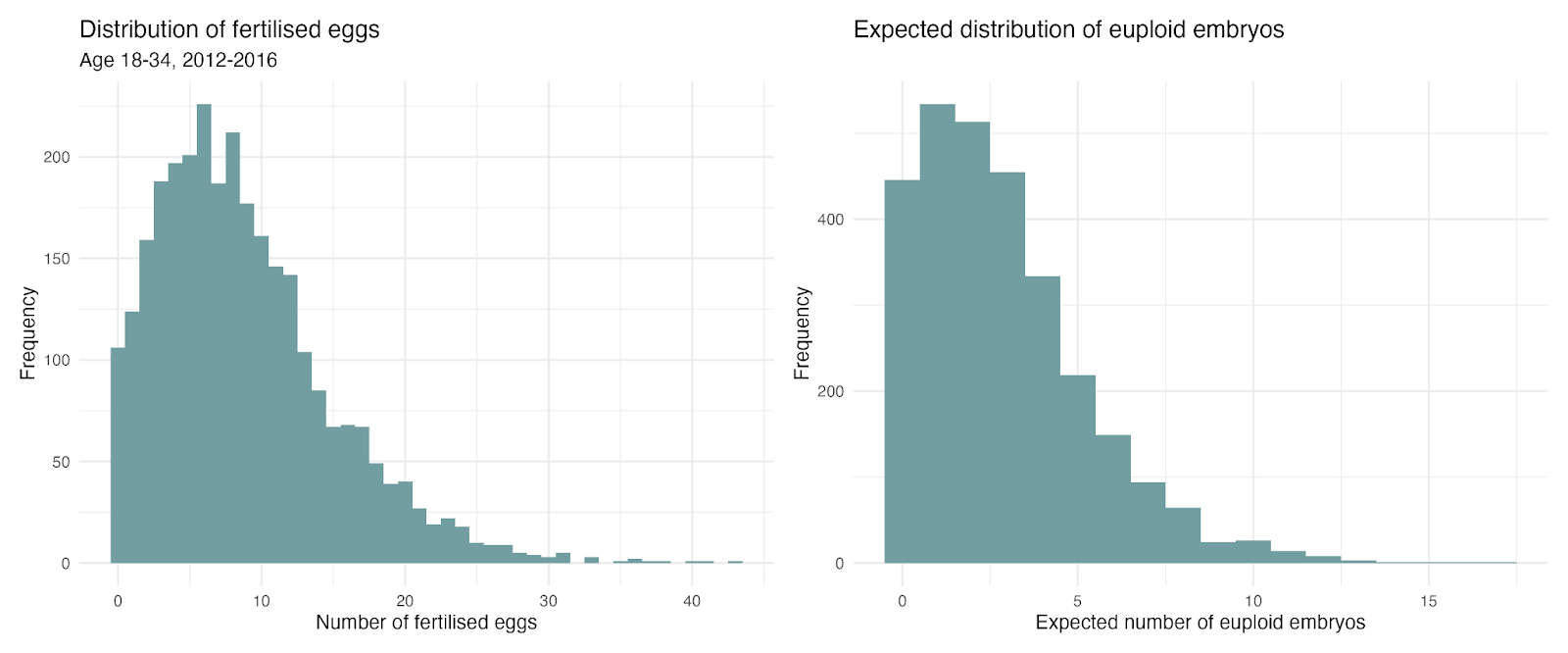
Figure 3. Distribution of the number of fertilized embryos and expected euploid embryos for women between 18 and 34 undergoing embryo freezing across clinics in the UK. Source: HFEA register data, 2012-2016. Own analysis. Note: To calculate the expected number of euploid embryos, we use the distribution of fertilised eggs and and simulate each egg having a 50% chance of turning into a blastocyst and each blastocyst having a 65% chance of being euploid, i.e. drawing from a binomial distribution.
 | A guest post by
|
So glad you put this together! Excited to point people to it as a resource. Had no idea about the importance of oxygen levels with embryo cultures and clinics neglecting to set low oxygen levels in their embryo culture chambers.
I really enjoyed this article and would like to read the Works in Progress magazine piece too, but the subscription is not available where I am (outside of Europe and the UK), and I wasn’t able to find an online article. Is there a stockist in Asia or Australia, or an online version?