
Manufacturing requirements are killing cell and gene therapy
Some of the most promising drugs are bottlenecked by a "boring" but incredibly important problem

Yesterday, ultra-rare disease company Grace Therapeutics announced it may be forced to shut down after the FDA requested a second manufacturing run before it can submit its new application for approval. This is a requirement the company says it simply cannot survive, as it would require another twenty million or so in funding. I explained in a tweet why the requirements the FDA has regarding this are absurd.
What I really want to bring home though is that the story of Grace Therapeutics is not unique by any means. Excessive manufacturing requirements are a pervasive problem, especially in the field of cell and gene therapy and they are killing countless of promising medicines before they ever reach patients. And they manifest at every stage: starting with Phase I, as explained here, all the way to post-approval.
In this post, I want to focus on a story that happened post-approval and illustrates how even when a drug basically cures cancer it can be very hard to commercialize and turn into a profitable venture for the company making it. The drug in question is Carvykti, a CAR-T cell therapy for multiple myeloma that I wrote about at length last week for Works in Progress. If you haven’t read that piece, the short version is this: Carvykti is, by most clinical measures, one of the most remarkable cancer therapies ever developed. It is a one-time infusion that has produced durable, long-term remissions, and in some cases what looks like an outright cure, in patients for whom every other treatment had already failed. A third of patients in its pivotal trial remained disease-free five years later.
And yet, despite all of that, the company behind it nearly had its commercial launch derailed. This, I think, is a very good case study on why the cell and gene therapy field is in trouble and how much of it comes down to excessive manufacturing requirements. I should also warn at this point that much of the information below is not public. Instead, it was assembled from interviews with experts and paywalled industry reports and investor calls.
How the Carvytki launch almost got derailed by manufacturing requirements
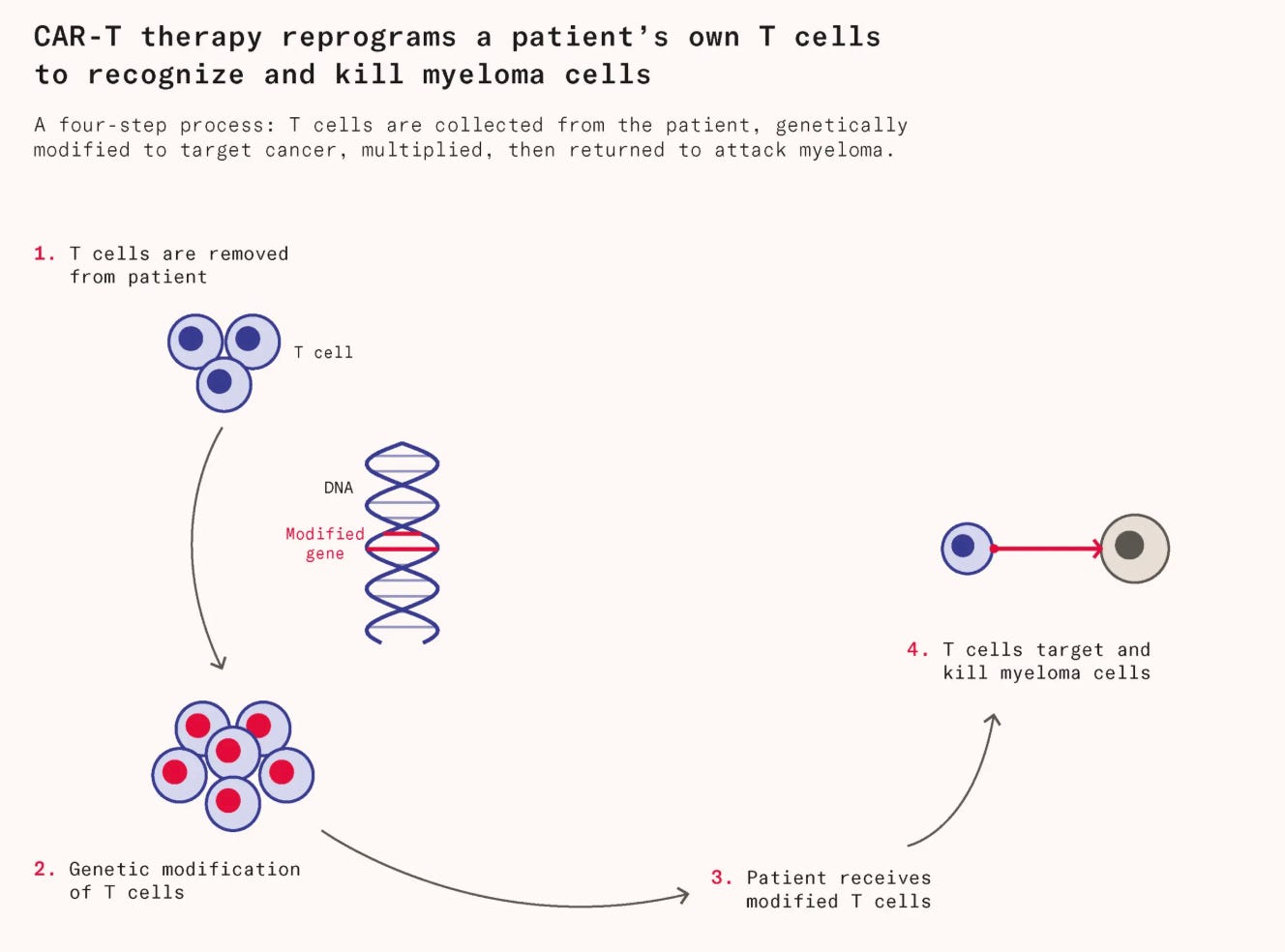
To understand how that derailment happened, it helps to first appreciate just how difficult these therapies are to make. CAR-T therapies are among the most complex products ever commercialised. Almost all approved CAR-T therapies are autologous, meaning cells must be extracted from each individual patient, genetically engineered, and returned to that same person, making the manufacturing process exceedingly difficult. Johnson & Johnson (J&J), the large biopharmaceutical company that co-developed Carvytki, faced additional hurdles in securing sufficient quantities of materials to manufacture the cell therapies, compounding an already complex situation.
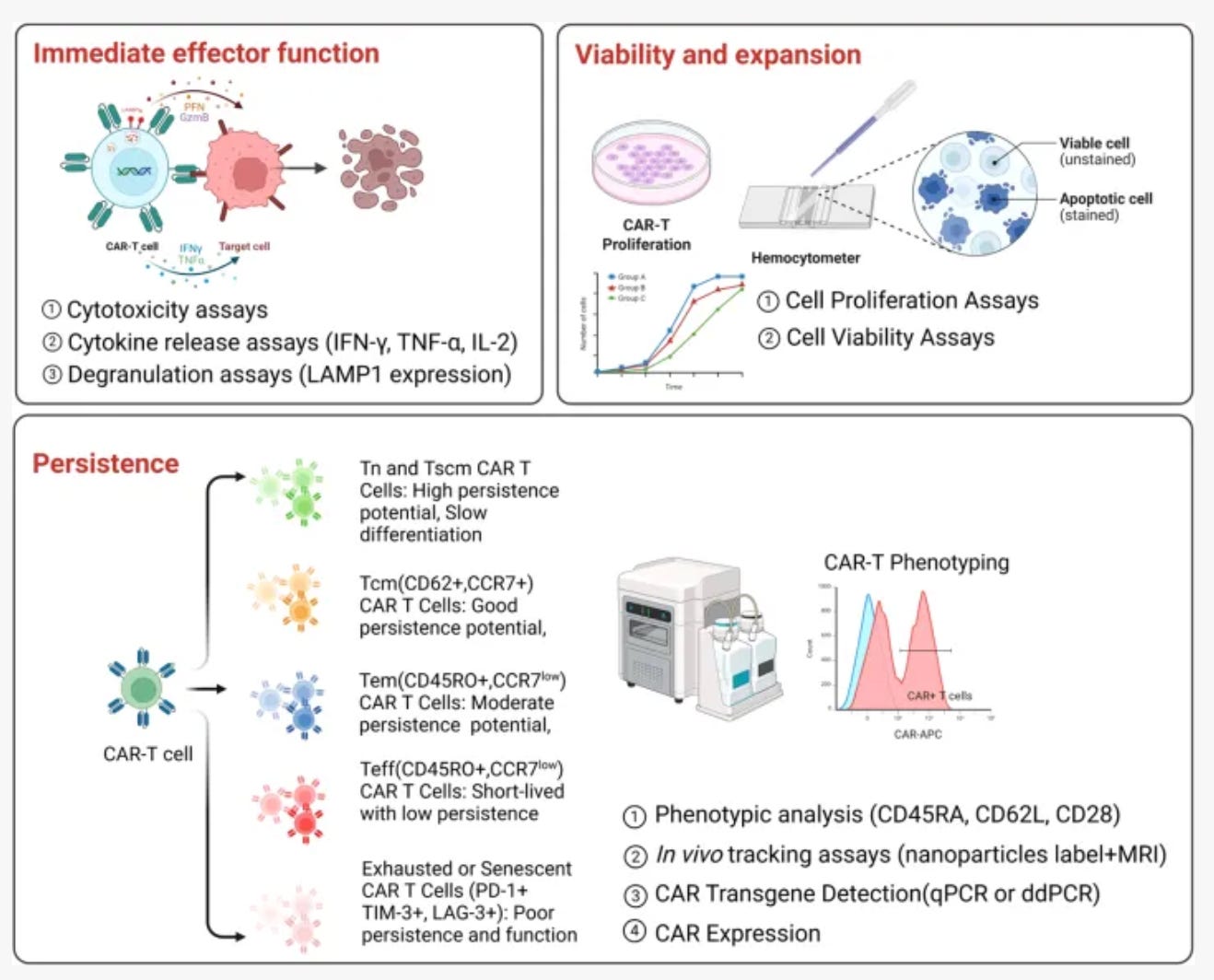
But perhaps the most surprising element hampering the therapy’s launch was a surprisingly high out-of-specification (OOS) manufacturing rate, estimated at 30 to 40% in the United States. Before any CAR-T product can be infused, it must pass a battery of quality-control tests. One of the most important is the potency assay, an in vitro experiment in which the patient’s re-engineered T-cells are placed in contact with myeloma cells, and their killing ability is measured. This test is meant to confirm that the therapy is genuinely therapeutic. A batch that falls short on any single measure is classified as out-of-specification, and usually cannot be administered.
These rates were far higher than anything observed during the clinical trials, for several reasons. In a real-world setting, patient heterogeneity is considerably greater than in the controlled environment of a trial, where eligibility criteria are designed to select for patients most likely to respond well and manufacture cleanly. At launch, authorised treatment centres were immediately overwhelmed with advanced, heavily pretreated patients and who in many cases would not have met the original trial’s inclusion criteria.
But the strangest contributing factor was one that originated not in the clinic or the manufacturing facility, but with the FDA. Somewhere between the trial phase and commercial approval, the FDA had tightened its potency assay thresholds. Legend Biotech’s leadership later calculated that if those stricter commercial standards had been applied retroactively to the original trial data, the out-of-specification rate would have risen from 2 percent to 18 percent. The therapy that had produced some of the most striking results in the history of myeloma treatment would, under the FDA’s new benchmarks, have looked like a manufacturing catastrophe.
Some industry observers were quick to point out the problems with this. The potency assay, first of all, is not a safety test. A batch that fails does not pose a risk to the patient, but falls short of an administratively defined threshold of activity. More importantly, the two parameters that most frequently triggered out-of-specification failures were traced not to genuine defects in the product but to minor technical artefacts in the assay itself, so noise in the measurement, as opposed to evidence of a non-functional therapy. Actual manufacturing failures, in which the product was biologically compromised or unusable, were exceedingly rare. This was, in the view of most people close to the field, a problem of regulatory stringency rather than one of therapeutic efficacy.
The human cost of this could have been significant. Imagine a 67-year-old with relapsed myeloma who has already been through five prior lines of treatment. While waiting for Carvykti, she is placed on bridging chemotherapy, a holding pattern designed to stop her disease from advancing while her cells are being processed. And, after weeks of deterioration and waiting, she is told that her batch has failed the potency assay by a few percentage points and sent home.
This was the fate faced by roughly a third of scheduled patients. To avoid such an outcome, rather than discard the failing batches, J&J took another approach. It routed the out of specification batches through expanded access, a regulatory pathway that allows patients to receive technically non-approvable products outside the formal trial structure. Companies cannot charge for therapies given through this route, meaning every out-of-specification batch was administered free of charge. In exchange, J&J collected rigorous outcomes data and compared results between patients who had received passing and failing product. What they found was there was no meaningful difference between the two groups.
Armed with that evidence, J&J returned to the FDA. When seeking approval to use Carvykti in earlier lines of treatment, the company combined the expanded access outcomes data with results from CARTITUDE-4, a randomised Phase III trial of 419 patients, and constructed a detailed analysis mapping manufacturing specifications directly to clinical outcomes. The conclusion was that thresholds had indeed been set too high. At this point, one might conclude that everything worked out, as patients received their therapy eventually through the expanded access program are measuring success too narrowly. But events of this kind are deeply damaging to a company’s profits, which reduces investor confidence and makes future development less attractive.
This would be less of a problem if it was isolated. But the Carvykti manufacturing saga is just one example of a failure that is, in fact, routine, especially in the field of cell and gene therapy. Manufacturing remains one of the largest hurdles in testing and bringing a cell or gene therapy to market. A 2022 retrospective study of 90 cell and gene therapy programmes entering Phase III found that 43 percent experienced major disruptions, and that 60 percent of those disruptions were traceable to CMC issues: potency assay failures, process changes, supply shortfalls. A single year of delay can cost a gene therapy developer between $100 million and $500 million in lost revenue and ongoing overhead.
Part of the problem is excessive regulatory conservatism, as the Carvykti potency thresholds illustrate. But another, less appreciated factor, is secrecy. Bespoke manufacturing processes confer genuine competitive advantage, and companies have little incentive to share hard-won lessons with rivals or with the contract manufacturing organisations that serve the broader industry.
Secrecy also applies to regulatory decisions and compounds the problem. Because the FDA rarely makes its earlier judgments on manufacturing specifications public, developers have little visibility into what the agency has accepted before. That gives specialist manufacturing vendors that drug companies depend on considerable leverage. Drug developers cannot easily benchmark whether a given requirement is truly necessary or whether a cheaper approach would satisfy regulators. As a result, vendors can charge for uncertainty. The result is an emergent ecosystem plagued by inconsistency and lack of transparency, where prices are difficult to challenge, and manufacturing costs remain higher than they need to be.
Compounding the problem is that assay standardisation is not especially attractive work for academia. Method harmonisation may be enormously valuable, but it rarely produces the kind of landmark paper or career-defining result that researchers are rewarded for.
Regulators themselves are aware of the problem that manufacturing poses to drug developers. In 2023, the FDA convened a high-level meeting with the Alliance for Regenerative Medicine and the American Society for Gene & Cell Therapy to focus specifically on potency assays. The white paper that followed recognised the structural dysfunction, but offered little in the way of a practical solution.
And although manufacturing sounds like a boring afterthought, the presence of such hurdles represents a major blocker for the field, as it makes an already scientifically risky field even more unattractive to pursue for investors. Carvykti is, by most clinical measures, a landmark therapy and has changed the outlook for patients with relapsed myeloma and built a credible case for moving cell therapy into earlier lines of treatment. Yet such commercial hurdles deter investors from investing in the space.
Investors read clearly into these signals and respond accordingly. Venture funding for the cell and gene therapy sector fell from $8.2 billion across 122 deals in 2021 to $1.4 billion across 39 rounds in 2024, a collapse of 83 percent in three years. A BioCentury analysis found the trend continued to worsen into 2025. These reports quote concerns over manufacturing requirements and general high manufacturing costs as a key reason behind the general bearishness surrounding the sector.
Until manufacturing and regulatory risks become easier to underwrite, capital will keep drifting away from one of the most promising technologies of the last century. The result is a loss for everyone. Some of the most promising cancer therapies of the next decade may take longer to reach patients, if they are pursued at all.
Is there any chance of running such a lab in the EU? Or are the rules as bad?
This is the unglamorous truth nobody wants to lead with: the science works and the manufacturing line is where it dies. A therapy that cures one patient in a trial but cannot be made reproducibly at scale is barely a therapy. Do you think the fix is mostly regulatory, or do we need genuinely new manufacturing platforms before these cures become routine?