
Reproductive health needs more hard science, not just more apps
Female and Reproductive Health are relatively popular buzzwords in the start-up space now; But all that glitters is not Gold: How much actual material progress are we making?
I was diagnosed with PCOS (Polycystic Ovary Syndrome) when I was 16 years old. I am not unique: it is thought to be the most common endocrine disorder in women of childbearing age in the US & the most common (albeit also among the most treatable) cause of infertility. Given this, you’d think we know a fair amount of stuff about it. Wrong! Even its exact prevalence is contested, with estimates ranging from 2 to 20% of women (the most likely estimate being somewhere around 10%). This uncertainty in something as basic as its frequency reflects a deeper issue: we don’t really know, at a fundamental biological level, what PCOS is. Different afflictions, with different prognosis, are probably being lumped together under a common name. This makes diagnosis & classification of PCOS harder: hence the uncertainty around its prevalence.
Back when I was 16, the possibility of one day having a child seemed very distant, so I did not give it much thought. As most other women diagnosed with this condition, I was given the contraceptive pill, which dealt with more immediate issues, like acne. All was fine. As I turned 26, however, I realised that my future family was something I had to think about - especially in the light of planning my career. So I decided to get myself checked once again and dig into all the information I could find: How much would PCOS impact my fertility?
What I realised, after going to 2 different doctors & reading the existing scientific literature, is that we know very little about reproductive health. There’s also been shockingly little progress in substantially extending female fertility and delaying ovarian ageing. This did not completely shock me: after all, I had delved into these topics before, albeit rather superficially, and my impression had always been that “we don’t know much”.
However, I think there is hope on the horizon, with new approaches to female fertility popping up. In this piece I hope to shine a light on the current state of female fertility & highlight some promising avenues of research, whether pursued in academia or commercial enterprises. I also want to point out what I consider to be distractions: areas that have received a lot of attention and hype but are not ultimately going to make a big material impact.
Some normative assumptions

This piece will focus specifically on female reproductive health. In the United States, among married women aged 15 to 49 years with no prior births, about 1 in 5 (19%) are unable to get pregnant after one year of trying (what is classified as infertility) and out of these, it is estimated that between 33% to 50% are caused by infertility of the female partner. Although male infertility also represents an area of increasing concern, it lies beyond the scope of this piece.
There are 3 pillars of improving female reproductive health that my essay considers worth tackling as soon as possible. From now on, I will refer to them by these numbers.
The pillars are:
Improving prediction of fertility to facilitate family planning
Improving treatments for existing infertility
Increasing reproductive span (the period of time a woman is fertile)
The contents of this piece are based on the normative assumption that all 3 of the outcomes described above are a positive and thus something worth working on. While I think almost everyone agrees 1 and 2 are unalloyed goods, there is more debate on whether 3 is desirable. This is not an essay that is primarily dedicated to discussing the social and moral implications of pillar 3. However, I think it’s worth briefly mentioning the objections to fundamentally altering the timeline of female fertility. If you are not interested in this, you can skip directly to the next section.
There is a growing movement within conservative circles centred around opposing the use of biotechnological interventions to alter biological realities (let’s call them bio-conservatives); something as ubiquitous as the contraceptive pill would classify as such an intervention. While I have not been able to find any article that directly opposes extending female reproductive span through biotechnology, I assume they would oppose it, given the tenets of their ideology. Bio-conservatism comes from such a fundamentally different place from myself, that there is little point in discussing it here. But if you’re interested to find out more I recommend the writings of Mary Harrington on this topic.
Instead, I will address some more concrete points:
A common criticism around increasing reproductive span is centred around the assumption that facilitating the delay of childbearing will create an incentive structure that will further discourage family building. Perhaps unsurprisingly, this comes from a conservative perspective: unshackled from the limits of their biology, women will live in a perpetual teenagehood even more so than they did before and further delay family formation. This point relies on a lot of assumptions that are hard to check, but my opinion is that we should seek to increase family formation through positive interventions (a more family-friendly/pro-natalist culture, increased involvement of dads/extended family in childrearing, more attractive maternity provisions), rather than seeking to limit women’s freedom and taking a reactionary approach. At the end of the day, if we don’t take these steps, TFR (Total Fertility Rate) is likely to continue decreasing regardless of whether we increase reproductive span or not.
Others point out that having kids later in life reduces the total amount of time one spends with their offspring and potential grandkids. To this I reply simply: people can freely choose how much they value cumulative time with their kids/grandkids over their life. Moreover, I think that if we are to achieve a dramatic increase in reproductive span, it is unlikely that in the process we wouldn’t also increase lifespan; this would automatically increase the time one spends with their kids. And, lastly, even small amounts of time added to reproductive span can make a huge difference in the defining decade that is the 30s; by contrast, they seem much less consequential in the grand scheme of one' individual’s entire life.
On my part, I start from the normative assumption that more control over one’s health and life is GOOD. In many ways, the life of a young woman is dominated by the spectre of her declining fertility: it creeps in into every decision she might make: from career, to location, to taking risks and choosing a partner. A relative liberation from such worries can be considered a good in itself and in my opinion what any feminist should focus on. In a way, I am coming from an ideological position opposing that of bio-conservatives. But ideology is hard to debate. Are there any concrete positives coming from extending reproductive span?
Firstly, most involuntarily childless women cite not having found the right partner as the reason for remaining childless. Thus, delaying the end of the reproductive span would allow this group of women a larger timeframe for finding partners to start families with. This seems undeniably good.
From a career perspective, as noted historian economist Claudia Goldin stresses, the gender wage gap is in large part a “motherhood gap”: the gap is much smaller for women without children. However, when women become mothers their earnings take a major hit & do not really recover. She has proposed solutions for this, including “changes in the labor market, especially how jobs are structured and remunerated to enhance temporal flexibility”. However, recent data points to the fact that generous childcare policies do not lead to gender convergence1. But it seems to me like a more fundamental solution is ignored, perhaps because it’s so outside our current grasp: enabling women to take control of their fertility and have kids later in life, when their careers are more advanced. A counterpoint to this is that childbearing cannot be indefinitely delayed and sooner or later these penalties will be incurred regardless of when childbearing happens. However, my hunch is that the 30-35 period, which happens to coincide with a decline in female fertility, is particularly important for establishing oneself as a professional and that women are at a particularly stark disadvantage because of this. Data supporting this hunch is hard to trust: studies showing that women who delay childbirth have better careers are highly confounded. Think of it this way: women who delay childbirth are also more likely to be the very ambitious kind, so it’s hard to say if having kids later is in itself causing better career outcomes. A clever study has recently attempted to get around this by looking specifically at the effect unplanned pregnancies have on careers: the “accidental” aspect serves the purpose of eliminating much of the confounding I discussed before. The article is not yet released in full, so it’s hard to assess it, but I suspect it will be an important addition to the literature. If true, this research bodes well: at least when it comes to careers, it shows that we needn’t even dramatically extend the female fertility window; Simply making sure most women are able to reliably get pregnant at ages towards the upper end of what could be considered the “natural spectrum” could potentially make a big difference.
And, to close this section, I’d like to stress another aspect: biological discovery is rarely a linear process; the line between treating infertility and extending female reproductive span is often blurred. It’s likely that advancements in the realm of treating infertility will have some spillovers and increase the percentage of women who can get pregnant at an older age; This goes the other way too: if we pursue the aim of increasing reproductive span we will likely find things that will impact infertility.
The current state
My impression that reproductive health is not valued proportional to what it deserves is supported by data from the NIH. This is a nice plot showing the funding by area of disease vs DALYs (Disability-Adjusted Life Years).

Briefly, DALY is a measure that has been introduced in the 90s with the aim of objectively quantifying the burden a particular disease places on a population. These scores are widely used to calculate the cost-effectiveness of medical interventions. There are numerous objections to DALYs and how they aim to quantify the burden of disease, but I think they are particularly bad at capturing the harm associated with infertility. Briefly, DALYs and QALYs (Quality- Adjusted Life Years, a “sister” method to DALYs), have been developed to capture the ability of an intervention to improve, extend, or save existing life. However, they represent a very poor conceptual framework for evaluating the value brought by new life and also underestimate the improvements on the parent’s quality of life from having a kid.
Think of it this way: How many people you know would sacrifice a few years at the end of their lives for the possibility to have kids at all, an event widely considered transformational? If we extrapolated from Q/DALYs, this number would be 0! Somewhat reassuringly, as this recent article shows, there is increased recognition of the fact that the measures we currently have poorly capture the value of creating new life.
Another metric we can look at apart from NIH funding is the number of publications that pop up on PubMed when using a specific keyword: for female fertility it’s 92000. By comparison, cancer comes up with 4 000 000 results!
Despite what I consider to be an under-prioritisation, I don’t wanna give the impression that nothing has been achieved on the fertility front in the past decades. Whereas no substantial progress has been made in fundamentally altering female reproductive span (pillar 3 in my classification), there have been improvements in treating some causes of infertility. Arguably, the biggest success story in this domain of the last few decades has been IVF. IVF is now used to increase chances of conceiving in a wide range of infertility cases ranging from those caused by ovulatory issues to endometriosis. The first IVF baby was conceived in 1978; Today IVF accounts for ~ 1-3% of births in US , numbers that speak to the positive impact it has had.
The success rates for IVF have increased substantially since it was first introduced. IVF used to have a success rate of only 6% per cycle when it was first introduced; This has increased to nearly 50% for women under 35 today. This is an undoubtedly dramatic improvement. A large proportion of this change is due to improvements in the culture media used for the embryos and the development of controlled ovarian stimulation, which allows multiple eggs to be retrieved per cycle. There is continued interest in improving the culture conditions of IVF to further increase efficiency, but as I discuss later on, I think this will have diminishing returns and more innovative approaches are needed at this point.
So what is there to hope for in the future? I will talk more about this in the last section of this piece, but female health generally, and reproductive health in particular, have recently started to get more attention. People have come up with innovative approaches to fund academic research in this underserved area. For example, AthenaDAO is a “decentralized community of researchers, funders, and advocates working to advance women’s health research, education, and funding”. They recently funded their first batch of academic research, specifically in PCOS and endometriosis. There is also investment coming from the private sector, notably Venture Capital firms, with companies like Conception securing large funding rounds. But not all that glitters is gold…
I am much less enthusiastic about the recent crop of companies falling into what could be broadly described as “Female Tech” (FemTech), one of the new buzzwords in the biotech start-up world. The reality is that most of the companies involved in female tech (very often coming in the form of apps) are “symptom-management” tools. To be clear: there is nothing wrong with apps. They can save money, time spent at the doctor and generally make life more seamless. But they are not really game-changers. Most importantly, they tend to simply recycle the existing, already scarce scientific information as opposed to generate new one. By their very nature they won’t bring substantial improvements to fertility; Instead their contribution to fertility is their attempt to “predict” it and thus help women with family planning (pillar 1). But as I explain next, even in this domain, they have not brought much innovation. Thus, despite the recent increase in interest that these companies have elicited, I think we shouldn’t lie to ourselves: Biology is hard and we need more research, not more apps.
To summarise, most of the advances so far have been done in the realm of improving the chances of conceiving for couples who would have otherwise been infertile (pillar 2). We have some imperfect measures of female fertility (pillar 1), which have nonetheless not increased in accuracy despite the recent proliferation of FemTech focused companies. On the other hand, there’s been no substantial advance on the pillar 3 front: fundamentally altering female reproductive span.
In the next part I will focus on highlighting the somewhat disappointing state of the current tools we have for predicting fertility & why I think FemTech is a distraction from actually trying to do the hard scientific work required for real progress.
A FemTech case study: Hertility Health
I sampled Hertility Health's £149 at-home Hormone and Fertility Test. The test sounded perfect for someone like me who has PCOS and a keen interest in starting a family. Like many app companies, they've made an impeccable website with a lovely colour palette and a design that screams "feminine but mature". I completed a series of their questions and an algorithm plopped out a "personalised hormone panel".

So how did the algorithm do?
Well… it recommended I test the same hormones that an endocrinologist in Romania did 10 years ago. The exception of AMH (Anti Mullerian Hormone), which is specifically supposed to measure fertility, and wouldn’t have been relevant when I was 16.
So overall this is a standard test that an endocrinologist would recommend to somebody with PCOS symptoms. I want to be clear: to the extent that this helps people avoid hours of waiting at a hospital or a doctor, it’s indeed a very good idea.
But quite unlike what is promised, it does not offer a very good estimate of fertility.
Why is that? Because, at the moment, we simply DO NOT have a very reliable way to estimate fertility, apart from the classic method: knowing the age of the woman. This is daunting, since age in itself is an imperfect measure.

I like this plot. It shows the extent to which age predicts the success of in vitro fertilisation (IVF). After 35, the success rate starts to decline, becoming incredibly low for over 44. This is mainly due to ovarian ageing, which leads to a decrease in quality of eggs (or oocytes). Ovaries are the organs that contain the oocytes, and they experience an accelerated ageing rate compared to other organs. But the question is, can a test provide any additional information on top of age?
Out of all the hormones recommended by the test, the best indicator for fertility is AMH (Anti-Mullerian Hormone). However, saying AMH estimates fertility broadly is, in my opinion, a bit of a stretch. AMH levels have good predictive value for a narrow problem: predicting functional ovarian response to stimulation during In Vitro Fertilisation, which can guide specialists administering this procedure (e.g with respect to dosage of stimulating hormones). To summarise, studies suggest AMH has some predictive value for the number of oocytes (eggs) retrieved during IVF. However, since a successful pregnancy depends on other variables than simply ovarian response, the existing evidence is much less clear on the extent to which AMH levels, independent of age, represent a full picture of fertility (which is what is implied by the phrase “Finally, get complete clarity with our at-home hormone and fertility test for women” on their website)
Some points:
Firstly, to the extent AMH reflects fertility, it seems to be predictive of IVF success, not of natural pregnancy. This is an important distinction, since the term "fertility" might be taken by many to mean "natural fertility" . As is the case with most epidemiological evidence, the results are sometimes in conflict, but aggregating studies suggests that the predictive value of AMH for natural
pregnancies is very poor.
So what happens when we restrict the problem space? If the question is "Can AMH predict successful pregnancy in response to IVF, independently of age? The data looks much better than for natural pregnancy, but the evidence is still mixed. In the best-case scenario, AMH offers moderate predictive powers that are greater for women older than 35 . When considering IVF itself, egg reserve – which is measured by AMH – is only a part of the picture.
Another eggy variable that has especial relevance to IVF success is egg quality. But with AMH alone, we're missing the part of the picture! You may be a woman who can retrieve a lot of oocytes, but age is quality, and that's why we see such a sharp decrease in IVF success with advancing age2.
But there’s another important aspect to this: AMH was first characterised as a promising marker for female reproductive health almost 20 years ago! Since then we have not come up with a better one. I think we should aim to do better than simply repackage relatively old science.
The future

The theme of what I just wrote is that age is the best predictor we have for success of assisted reproduction, with success rates starting to decrease after 35. For natural conception, it’s a bit harder to establish the exact success rates (harder to monitor), but there is a general consensus that fertility also starts to decrease after 35. The main problem women tend to face is a problem of priorities; women who really desire to have kids at some point in their life have very little way to know if they're among the unfortunate group who will have difficulty conceiving after 35. Simply put, age reigns supreme when it comes to prediction. But must it?
What if we had additional metrics to inform women's decisions so they know they ought to start earlier or that they might be able to start later?
I will be honest: I think this is awfully hard. Although progress is being made in understanding what determines oocyte quality, I think decades of relative neglect means that we are a long time away from this (but I hope I am wrong, and hey there are some very cool recent studies related to this!). There are some positive signs in this direction. For example, this recent study identifies genetic variants involved in DNA damage response as important for ovarian ageing. The problem is that, even if we understood what determines oocyte quality, the path from that to an actually informative and non-invasive test that women could take is an arduous one.
There is another way: Instead of aiming to predict biology, we can try to modify it. We wouldn't need to worry about oocyte quality if we could extend the fertility window. In some areas of medicine, prevention and prediction are preferable to treatment (e.g., oncology); reproductive biology is in a situation where the opposite is decidedly true: being able to circumvent the biological limits of female fertility would be far more impactful than predicting if a woman will become functionally infertile in five rather than eight years. We don’t need to modify biology only when it comes to extending reproductive span (pillar 3); it’s also very important for couples who are infertile to begin with (pillar 2). So I hope that even those who don’t find the idea of extending female reproductive span that appealing will at least agree improvements in technologies aimed at infertile couples are good;
Improving IVF (In vitro Fertilisation): Although IVF has progressed a lot, it is still far from perfect: after 3 cycles the success rate is ~ 67% and can rise to about 70-90% after 8 cycles for women under 35; For women between 35 and 40 the success rates are much lower, and for above 40 they fall even more dramatically: less than 10% success rate for over 44s even after multiple cycles.
So there is still quite a lot of work to be done in terms of improving these numbers. As mentioned before, a lot of improvements so far have been due to wrk on optimising the embryo culture media, but future focus on this area is likely to yield diminishing returns. As a result, some companies are moving beyond that: for example, Notify does overstimulation of remaining primordial follicles3; this is a last resort strategy, as it comes with the risk of early menopause.
Another promising new area is In Vitro Maturation, which is what Gameto & Vitra Labs are attempting to do. The TLDR on In Vitro Maturation is that instead of using mature oocytes, as current IVF protocols do, it retrieves immature ones and then matures them in vitro4. How would this help? Firstly, it would improve the efficiency of IVF by using immature eggs and thus solve at least some of the cases where IVF fails. Secondly, using immature oocytes would allow for minimal or abbreviated ovarian stimulation cycles. This would be a crucial improvement for women who are suffering from severe negative side-effects as a result of ovarian stimulation (e.g. Ovarian Hyperstimulation Syndrome).

The process of maturing oocytes in vitro involved retrieving immature oocytes and then co-culturing them with so-called “supporting cells”. These mimic the natural environment the ovary provides for oocytes to mature in. Taken from the Gameto website. Increasing female reproductive span: An obvious way to increase female reproductive span is by delaying ovarian ageing.
Unfortunately, we have a rather poor understanding of what leads to ovarian ageing; That does not mean there are no attempts to slow it down or reverse it .
For example, a start-up called Jumpstart is using NMN derivatives to enhance oocyte quality either in vivo or in vitro - culture media based on recent findings that NMN can help rescue female infertility. There is also hope that some of promising avenues in broader ageing research could be repurposed to aid in combating ovarian ageing. Most notably, rapamycin, a compound that is currently in clinical trials for its potential to delay general ageing symptoms, has shown some promise towards ovarian ageing. Of note, all these strategies have only been tried in animal models, so whether they would successfully translate to humans remains a big question mark.
So if “de-aging” ovaries is so hard, are there any other avenues that are being pursued?
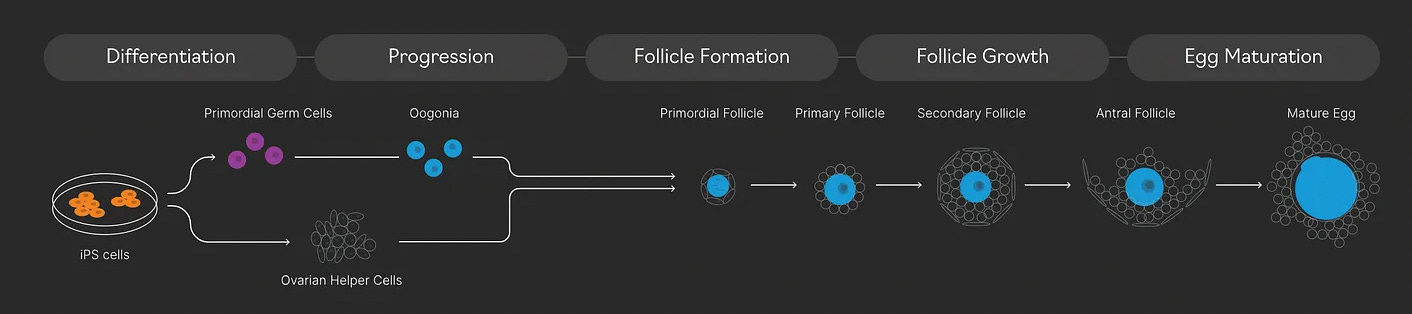
If you cannot fix something you can create it anew. Sounds wild to apply this principle to oocytes, but this is exactly what companies like Conception are trying to do; The aim is for blood cells from an individual to be collected, dedifferentiated into a stem cell state (iPSCs - induced pluripotent stem cells) and then converted into functional oocytes that can then be fertilised. All outside the woman’s body (in vitro)! In short, they are trying to create eggs in a dish from blood. These would behave as “young” eggs, even if the initial blood cells were collected from an older individual.

Conception aims to create eggs from iPSC cells, themselves derived from blood cells of mature people. Picture taken from Conception website The caveat to this approach is that it’s well… very hard to achieve. Other cell types have been differentiated in this way from iPSCs, and indeed this is the main method used to obtain cell therapies (involved in eg. cancer treatment) at the moment. But oocytes are a particularly tricky cell type, not least because they have such a complex developmental trajectory, with multiple stages.
So, given how hard this task is, what gives researchers hope it can even be achieved? For starters, there has been a lot of progress in obtaining mouse oocytes using this method. This was mainly kickstarted in academia, by 2 Japanese groups (Saitou and Hayashi), both of whom had trained at some point with the eminent British developmental biologist Azim Surani. I recommend this review & this very recent paper if you are interested in some of the latest developments in the academic space5. Achieving oocyte differentiation from stem cells is not useful only from the perspective of prolonging fertility. It would also offer researchers a very rich resource for testing interventions against infertility for a wide range of ages (again we see the interaction between pillars 2 and 3).
If this approach works, it would have dramatic impacts: not only leading to dramatic fertility extension, but also potentially allowing same-sex couples to have kids. Unfortunately, even if it does eventually succeed, it’s somewhat unlikely this will happen in the immediate future. Henry Greely, a bioethicist at Harvard University says that his expectation is that this technology is going to be available in about 15 years. This apparently large period of time makes sense when you consider that even if we do succeed at creating human oocytes in a dish, there are numerous safety implications; We would have to first try and test this in animals, starting with mice and probably continuing with monkeys, to check that embryos developed using this technique develop normally. Considering all these, and the still somewhat incipient phase we are at in terms of the science itself, 15 years might actually be an optimistic estimate.
The high-risk nature of this approach is probably why Gameto is not putting all their eggs in one basket (pun intended): while their final aim is to also derive mature oocytes from stem cells, they are trying the safer, more achievable In Vitro Maturation route in parallel. Egg maturation is after all the final step in obtaining functional oocytes from stem cells, so they are killing 2 birds with one stone! It seems like Vitra Labs is following a similar strategy,

There is a common thread in the approaches I am excited about: whether happening in academia or commercial settings like start-ups, they are ambitious and aim to actually change the Science, not just wrap existing knowledge in a commercially lucrative product. Given the relative underprioritisation of fertility research, we are still far away from solutions. We might be 1 or 2 or even more decades away from the ambitious goal of creating a oocyte in a dish. But we have to start somewhere. And if these solutions are not gonna be accessible to me, I want them to be for my daughters. Indeed, I hope they will be able to break the “age ceiling”.
The caveat is that this is just one study, so the literature would need to address this further in order to establish the extent to which expanded childcare reduced the gender wage gap
the other complication here is that egg reserve itself decreases with ageing. So in practice most women with a low egg reserve will also have low egg quality
A primordial follicle is a structure found in the ovaries and represents the earliest stage of follicular development. It contains a single immature egg cell (oocyte) surrounded by a layer of flattened cells called granulosa cells
in vitro studies are conducted using components of an organism that have been isolated from their usual biological surroundings; in this case the oocyte is being cultured outside the woman’s body, in a biological culture dish
Not as burdened by worries about intellectual property, academic labs are often much more transparent about the latest developments than companies so if you are interested in the scientific details, I recommend checking out academic papers
Great post.
My guess is that breakthroughs in anti-aging research (in general) will automatically lead to an extension of female reproductive span.
Very informative! Thanks for writing it.