
Autoimmune therapies: an inspiration for anti-aging therapies?
On how anti-aging therapies could piggyback on autoimmune treatment strategies in the same way the latter piggybacked on advances in cancer therapies

Disclaimer: This is all very speculative
The simplest definition of autoimmune diseases is as a class of pathologies wherein the immune system starts attacking the self; something that, in healthy individuals should not happen, due to the body “training” immune cells in something called “self-tolerance”. Behind this very broad definition though, hides a labyrinthine complexity. Autoimmune conditions differ wildly in phenotypic manifestation: ranging from relatively “mild” psoriasis to conditions that can have a ~ large impact on life expectancy like type I diabetes (approx 10-12 years). They are heterogenous in terms of the organs affected: some autoimmune conditions are relatively “localised” (e.g. inflammatory bowel disease (IBD)), while others are systemic1 (e.g. systemic lupus erythematous) and they can involve a variety of immune cells (B cell, T cells, monocytes etc).
Historically, autoimmune diseases have been treated with non specific therapies like corticosteroids: these are drugs that broadly suppress immune function; because of this, they have limited efficacy and come with a host of unwanted side-effects, including a high susceptibility to infections.
In recent years, however, biotech and pharmaceutical companies have become increasingly interested in more targeted therapies against autoimmune diseases: molecules that are directed towards specific immune cell populations (e.g. T cells or B cells). In many ways, this can be seen as a “drug repurposing” effort, after the success of a host of modalities in treating blood malignancies2. After all, in a blood cancer you are trying to destroy an immune cell population gone rogue — not too dissimilar from what one’s aim is in autoimmune conditions! Trying an already tested approach in another type of disease that shares a key commonality seems like the next logical step. And that’s exactly what’s happening at the moment.
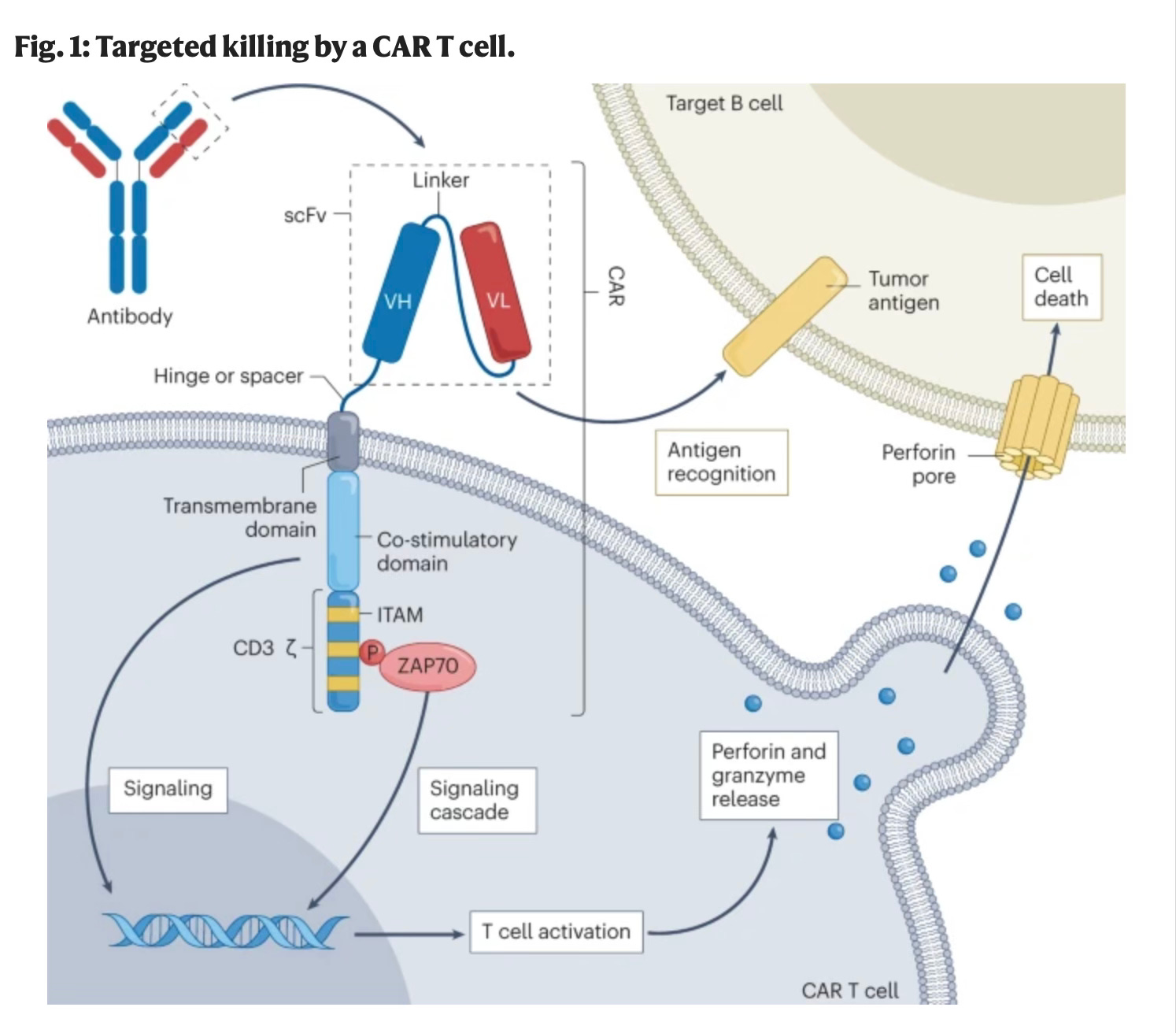
After antibodies had their moment, currently the “hottest” modality that is being repurposed from cancer to autoimmune diseases is perhaps CAR-T cells (Figure 1). These have already been transformative in blood cancers (e.g. Brexucabtagene autoleucel or Tecartus achieves 63% complete remission rate in mantle cell lymphoma3 ). The excitement related to CAR-T in autoimmune disease was spurred by a study on just five patients with treatment resistant systemic lupus erythematosus (SLE), a debilitating autoimmune condition, published in Nature Medicine in 2022. What this study lacked in numbers of patients, it more than made up in terms of results: the CD194-targeted CAR-T cells, which basically attacked most of the existing B cell population in the treated patients, led to drug-free remission. This was true even after the B cell compartment was repopulated with new ones. In context, these are very promising results: not only do they point towards a potential “cure”, but the fact that repopulation of B cells does not lead to disease relapse, suggests that patients do not have to suffer the consequences of long term immune suppression, as seen with corticosteroids: they just seem to develop new, better functioning B cells post this very harsh treatment. Of course, such small studies have to be treated with caution. However, subsequent investigations (also in small numbers of patients) showed similarly promising results in other autoimmune conditions, including systemic sclerosis and idiopathic inflammatory myositis. These very optimistic results have spurred larger scale clinical trials (Figure 2).
Autoimmune diseases are in some sense piggybacking on years of research done for oncology indications. And they will continue to benefit, in the future, from all the advancements that are currently being made in achieving more specific targeting of blood cancers.
One problem with many CAR-T cell therapies at the moment is that they are broadly attacking all cells expressing a specific antigen — this is quite a “blunt tool”. For example, CAR-T cells targeting the CD19 receptor can cause severe side effects like neurotoxicity or cytokine release syndrome. For patients with relapsing cancer, which face short survival timelines, such risks might pass cost-benefit analyses; but for autoimmune conditions, however life impairing, these side-effects can be real detractors. Fortunately, the oncology field has also given rise to companies like Outpace Bio or SentiBio, which are pursuing more sophisticated and precise strategies: using protein engineering techniques, they are aiming to create CAR-T cells that only get activated when specific combinations of antigens are present on the surface of a cell using logic gates5 . This would allow the targeting of ever smaller and more relevant cell subpopulations. In the meantime, techniques like single-cell RNA sequencing (scRNAseq) will allow more precise identification of relevant immune cell subsets, although determining causality will still remain a challenge6. OutpaceBio is also pursuing a strategy that would allow precise cytokine7 release only at the desired site, a way to prevent the potentially fatal side effect of cytokine release syndrome.
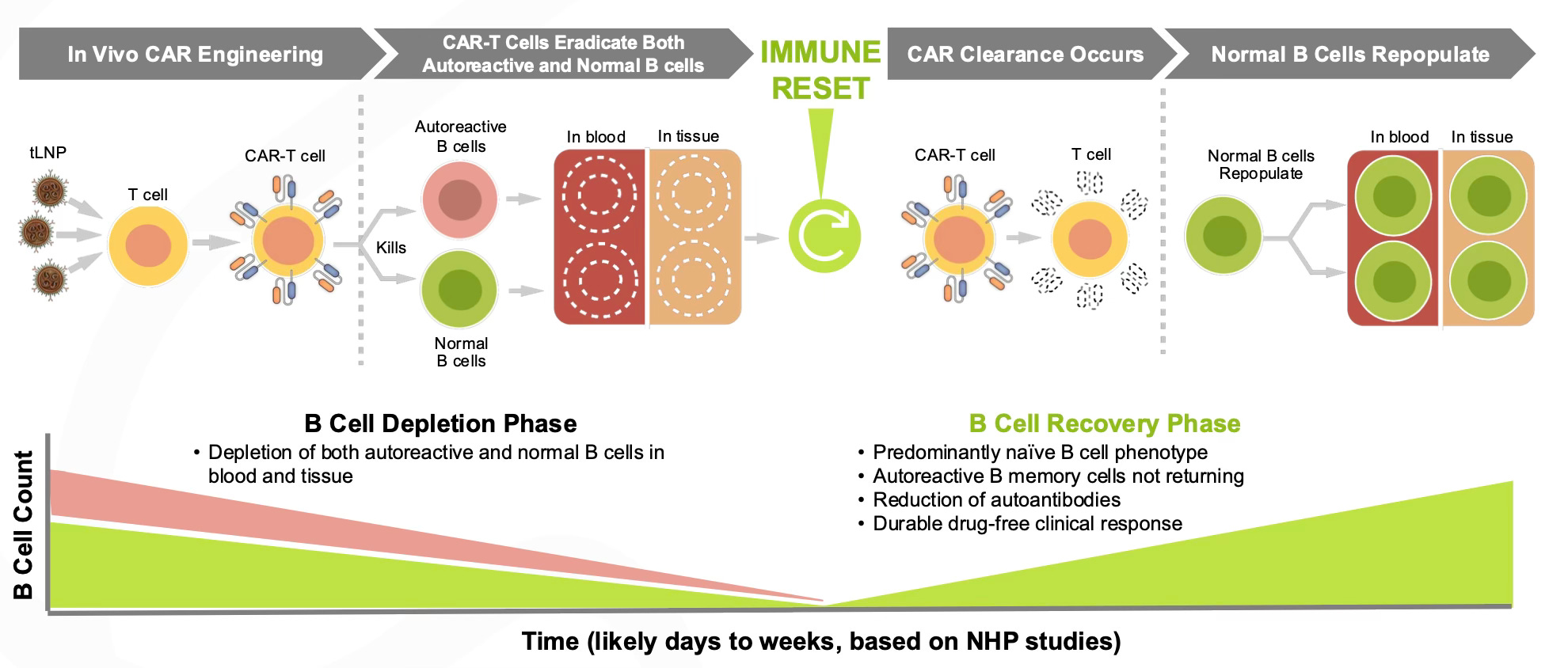
Another problem with current CAR-T therapies is that they require lymphodepletion, usually involving chemotherapy to remove existing immune cells, in order to “make place” for the CAR-Ts, which would otherwise be “outcompeted” by the patient’s existing T cells. This is of course very taxing on the body and there is evidence chemotherapy increases the risks of further developing malignancies down the line. Yet this is another problem that companies are working on solving — for example Capstan Therapeutics has raised a 175$ million Series B from leading investors like RA Capital to pursue in vivo CAR-T engineering. That means targeting the T cells of a patient with mRNA to express the required CAR in vivo, which would mean no lymphodepletion is needed8 (Figure 3).
Notably, Capstan is specifically focusing on autoimmune diseases9, which suggests that we are quite deep into “engineering CAR-Ts for the specific purpose of autoimmune indications” territory. Of course, all this has to be taken with a grain of salt. There is no incentive for start-ups like Capstan or Outpace to disclose the issues they are facing and we are yet to see their promised technologies work. And Capstan’s value proposition is so “big if true”, that them not getting acquired for a formidable sum in the following years will look bearish to me. What we can observe though is clear interest and work in the space, which seems to have convinced some top biotech investors10.

And CAR-Ts are just one of the ways in which autoimmune diseases are benefitting from advances in cancer treatment. Other modalities from oncology that show promise include bispecific antibodies, or antibodies that bind two targets at the same time. Overall, one can say the field of autoimmune disease has greatly benefitted from advances that were largely driven by the pursuit of therapies for blood malignancies. I believe that we might see something similar in the treatment of aging related disease.
My prediction is that at some point, the continuous development of ever more specific and efficacious molecular tools for depletion of certain immune subsets, driven first by oncology and then increasingly by autoimmune indications, will meet a better understanding of the ways in which the immune system is implicated in systemic age-related dysfunction. The growing importance of autoimmune indications is particulary important, as these demand higher standards of safety and specificity than cancer, which will incentivize companies to optimize on these dimensions. These will be highly beneficial for aging-related diseases like atherosclerosis, which already benefits from existing treatments, hence specificity and safety are needed. Furthermore, if we ever aim to do this preventatively (deplete pathogenic immune cell populations in the absence of overt disease), these two properties become even more important. So to summarize, the way I see the direction of positive spillovers is:
Blood cancer therapies → autoimmune therapies → aging therapies focused on immunosenescence
But, before getting into more details, let’s establish some premises. Firstly, that immune aging is very important for systemic aging.
Immune aging is very important
I have long believed that out of all types of aging, immune aging is the “Queen” of all. This is because, as blood circulating entities, immune cells interact with virtually every tissue, so immune senescence reverberates throughout the body. Perhaps the earliest hints that point towards the importance of immune aging to the decline in function across the entire body come from classic heterochronic parabiosis studies —in which young and old mice share a circulatory system. These revealed that “young” blood leads to younger phenotypes across multiple organs in older animals, including the brain (here and here); conversely, “old” blood accelerates aging features in young animals. Although the precise pro‑aging factors remain elusive, aged pro‑inflammatory immune cells are leading suspects.
Why might they be the prime suspects?
The first obvious answer is that they are circulating blood cells. The second answer refers to a phenomenon called “inflammaging”. We know that as the immune system ages, its performance declines, which translates for example in worse responses to vaccination and infection in elderly individuals. Paradoxically, it also drifts into a state of chronic, low‑grade activation known as “inflammaging”. Even in the absence of overt illness, older adults typically carry higher blood concentrations of inflammatory proteins—interleukins (IL‑1, IL‑6, IL‑8, IL‑13, IL‑18), type I interferons (IFN‑α, IFN‑β), tumor necrosis factor (TNF) and its receptors—as well as C‑reactive protein, transforming growth factor‑β, and serum amyloid A. Another hallmark of dysregulated immunity is the rise in antinuclear autoantibodies11 (ANA) with age — these are self-reactive antibodies commonly seen in autoimmune diseases. Perhaps one could describe all this, at a very high level, as an increase in entropy in the immune system with age: somehow worse at doing what it’s supposed to do and bad at doing what it is supposed to do.
More direct links between immune cells specifically (and not just blood generically) and aging come from studies in mice. For example, deleting the DNA‑repair gene Ercc1 specifically in hematopoietic stem cells, which are the precursors to all other immune cells, drives their senescence and triggers premature aging in multiple organs, whereas transplanting youthful immune cells dampens these effects. Similarly, inducing T‑cell–specific loss of a mitochondrial‑stabilizing protein in mice induces systemic frailty—neurologic, metabolic, muscular, and cardiac—through chronic TNF‑α‑mediated inflammation; blocking this inflammation reverses many deficits .
These are very interesting studies (from 2021 and 2020 respectively) that are certainly indicative of an important role of immune aging in systemic dysfunction, but they have a severe limitation: to “age” the immune system in these mouse models, the authors resort to very “extreme interventions” like deleting an important DNA repair gene or a mitochondrial protein. Yet a recent paper from 2024 does not suffer from such limitations: the authors show that in otherwise normal, old mice aging leads to emergency myelopoiesis (or overproduction of cells of the myeloid lineage, like monocytes) and an enhanced production of interleukin-1α (IL‑1α ) —a pro-inflammatory cytokine, from progenitor myeloid cells. These IL‑1α producing myeloid cells accumulate in lung tumours and stimulate its progression through suppression of other, positive anti-cancer immune responses. Blocking IL‑1α production using an antibody (a common therapeutic strategy in cancers), also slowed the growth of lung, colon and pancreatic tumours.
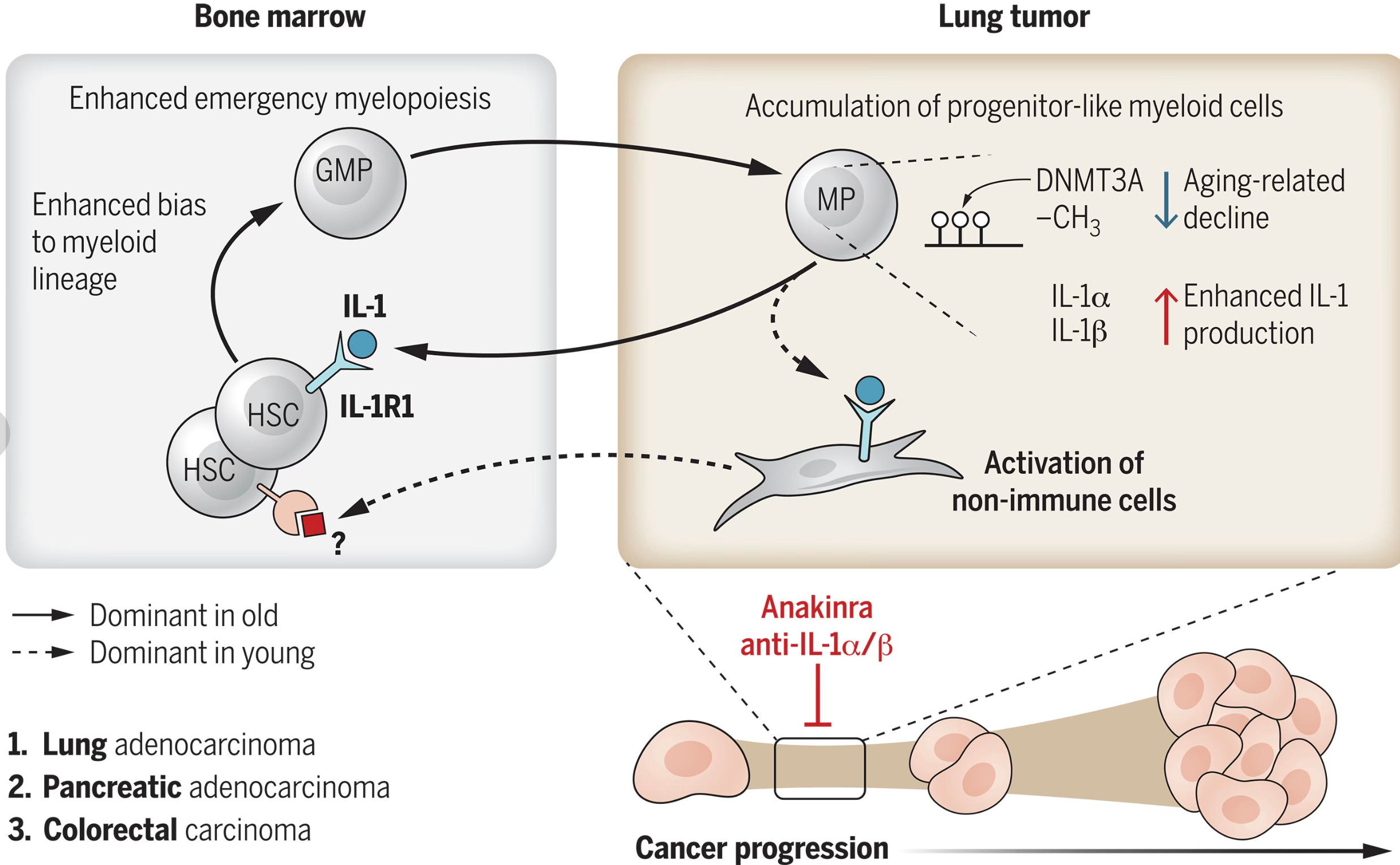
But this is about cancer, not systemic aging! Well, it’s worth mentioning aging is one of the most important risk factors for cancer development, with those over 65 bearing more than half of the cancer burden in the US. And non–small-cell lung cancer (NSCLC) is one of the most associated with aging cancers out there — which is precisely why the authors of the study focused on lung cancer. To further support this study, another recent paper in mice showed that depletion of myeloid-biased hematopoietic stem cells led to a more phenotypically youthful immune system.
Ok, ok but this is in mice! We have cured cancer in mice so many times. How are these findings relevant?
Well, such in-depth studies are mostly possible in mice. But besides that, there are two interesting findings in this study that point to its relevance to humans. Firstly, in mice, this overproduction of IL‑1α is driven by an age related decrease in the activity of a protein called DNA methyltransferase 3 (Dnmt3a). In humans, we observe somatic mutations that impair DNMT3A function and the frequency of cells carrying such mutations increases with age. This is all part of a phenomenon known as clonal hematopoiesis of indeterminate potential (CHIP), which I have already written about. CHIP has been shown to be associated with an increased risk of age-associated diseases, including, most prominently, cardiovascular disease. Secondly, the authors mined human existing publicly available scRNAseq human data and found expression signatures of the proposed pathogenic IL‑1α secreting cells among the monocytes that accumulate in human lung cancers. Thirdly, myeloid bias (a switch to production of cells of myeloid lineage) with aging is also seen in humans.
And, if studies in mice do not convince you, there is accumulating evidence (from humans) regarding the importance of so-called “chronic inflammation” in a host of age-related diseases including cardiovascular disease, dementia etc.
On long covid and autoimmunity
A few months ago I wrote a thread in which I explained why findings about post SARS-Cov2 vaccination syndrome are not what people made them seem to be. Writing this thread led me down a rabbit hole of reading about exposure to SARS-Cov2 antigens12 and the potential mechanisms behind long COVID — the disease whose very existence has been questioned so vehemently by many. One common “meme” on the internet (and in broader society) is that the higher prevalence of this disease in young women is just proof that it’s somewhat of a “fake disease” — just a psychosomatic manifestation of the higher anxiety that is prevalent among this demographic. The fact that “long COVID” has somewhat diffuse, hard to pin down or characterise via “hard measures” symptoms, makes the conversation even more difficult. Commonly cited manifestations of long COVID include: fatigue, shortness of breath, joint pain, insomnia etc. The nature of these symptoms means it’s a condition that’s easy to dismiss: after all, we cannot measure “fatigue” on a Computer Tomography (CT) scan like we do with cancer. Furthermore, they can be abused by bad actors and used to justify leaves of absence. But, in the majority of cases, as many people who have met actual long COVID sufferers know, the idea that this is just in young women’s imagination is nonsense.
There is something else that young women are predisposed to, besides anxiety: that is autoimmune diseases. And the group of Dr. Akiko Iwasaki, a very well-known immunologist, who is behind the post vaccination syndrome study I mentioned above, found something very interesting: individuals with long COVID, particularly those with neurological symptoms, often produce diverse and functional autoantibodies (AABs)— which are specific of autoimmune diseases, but also, as mentioned in the previous section, accumulate in the blood of healthy elderly people. Using a human proteome array, the researchers identified that these AABs frequently target proteins in the nervous system and correlate with symptoms such as brain fog, headache, and dizziness. Now, Iwasaki is looking into other post-acute viral syndromes with similar symptoms to long covid, including post-treatment Lyme disease and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).

Purified IgG13 from Long Covid patients reacted with both human and mouse neural tissues, including the pons, sciatic nerve, and meninges. When these IgG samples were transferred to mice, they induced symptoms similar to those reported by the patients, such as pain sensitivity, muscle weakness, and coordination issues. Mice injected with long covid patient IgG showed biological changes, including small fiber neuropathy, supporting a pathogenic role for these antibodies. The study suggests that autoimmunity may underlie a subset of Long Covid cases and that targeting AABs could be a therapeutic strategy. It could also explain why young women are both more likely to have long covid and autoimmune conditions: and underlying predisposition could underpin both.
Ok… but what does that have to do with aging? Well, it’s related to two concepts I mentioned in the second section of this essay: firstly, the broad phenomenon of “inflammaging” or chronic inflammation, which is thought to be a hallmark of immune aging and the accumulation of autoantibodies in the blood of “healthy” elderly people (two phenomenona that I think are related).
Viral exposure, autoimmunity and age related diseases
This is where things become very speculative.
Like in many other age-related pathologies, the role of inflammation or to use a more precise term, “improper activation of immune cells” in cardiovascular disease, most notably atherosclerosis, is being increasingly recognised, including by top leaders in the field, like Prof Peter Libby. I have copied exactly his explanation from one of his latest reviews on the topic in Figure 5. Interestingly, the two most successful and researched treatments for atherosclerosis (statins and various ways of inhibiting/downregulating PCSK9 — a protein involved in lipid metabolism) involve cholesterol control, with relatively little attempts to precisely control immune cell populations.

Against this backdrop of an increasing recognition of the role of inflammation in atherosclerosis (which is, of course, another age-related disease), my interest was piqued by a recent study analysing CD8+ T cell14 populations in human coronary plaques15.
The study found that CD8+ T cells within plaques are clonally expanded and often specific to viral antigens, including influenza, (Cytomegalovirus) CMV, (Epstein-Barr Virus) EBV, and conserved coronavirus epitopes. Epitopes are the specific parts of antigens that are recognized and bound by an antibody or a T cell receptor. Clonal expansion of T cells refers to the process by which a single T cell that recognizes a specific antigen rapidly multiplies into many identical cells to mount an effective immune response — overall the findings above suggest that these T cells had been stimulated to expand by the above mentioned viral infections.
These virus-specific T cells were most enriched in fibroatheromas, a stage associated with plaque instability and rupture. Notably, many of these T cells remained in the plaque despite the absence of active infection, raising questions about their persistent activation. Through sequence analysis, the researchers discovered that viral epitopes recognized by these T cells shared amino acid and nucleotide similarities with self-proteins expressed in vascular smooth muscle cells (SMCs), endothelial cells, and cardiomyocytes. As explained in the caption for Figure 5, the interaction between pro-inflammatory T cells and SMCs has been postulated to contribute to plaque progression. These findings suggest a potential mechanism of molecular mimicry, where immune responses initially targeting viruses cross-react with self-tissues, in autoimmune-like fashion. In vitro experiments confirmed that T-cell receptors (TCRs) from the plaques responded not only to viral peptides but also to self-antigens like TSPAN17 and Zip9. Such cross-reactivity provides a possible explanation for viral-triggered cardiovascular complications, even in previously infected or vaccinated individuals.
The findings also align with observations that autoimmune conditions elevate cardiovascular risk. These data imply that a subset of virus-specific T cells may misidentify vascular proteins as foreign, contributing to chronic inflammation and plaque progression. Overall, while not conclusive, the study supports a model in which viral exposure may initiate or exacerbate autoimmunity within atherosclerotic plaques.
Ok… so what am I suggesting here? I have presented only two studies so far — they both suggest a connection between viral exposure and triggering of a low-grade autoimmune-like response. In the first case, associated with long COVID. In the second case, with an age-related disease. But let’s recap some of the earlier stuff I mentioned: the phenomenon of “inflammaging” or low-grade aberrant immune activation with age, as well as the clues regarding its importance in driving systemic aging. I believe there is a possibility that accumulated exposure to viral infections with age could be responsible for “inflammaging”. In other words, that, in the long run, we are all subclinical sufferers of long COVID (or long EBV, long CMV etc). For some, this flares up very blatantly. For most, accumulated exposure to various viral infections merely leads to a progressive increase in these autoimmune-like, pro-inflammatory cell populations, which in sufficient numbers, end up impacting a whole range of age related diseases.
There are other pieces of evidence that antigen exposure produces a pro-inflammatory potentially self-directed response: for example, individuals with HIV, even those on antiretrovirals, are more likely to suffer from cardiovascular diseases. And let’s not forget other recent results that took the scientific world by surprise, like the recent link between EBV infection and multiple sclerosis (a full-blown autoimmune condition).
This is of course, all highly speculative. However, you do not need to believe my theory that links viral exposure, autoimmunity and aging to think that treatments for autoimmune diseases might lead to “positive spillovers” into aging-related pathologies. Instead you need to buy a much narrower claim: that there are subpopulations of aberrant immune cells that are causal in age-related decline and that depleting those would lead to amelioration of a host of these age-related phenotypes. This is a much narrower claim, which at this point I think has pretty solid evidence.
The good news is that we have been developing ever more precise tools to target blood malignancies. This has led to a “positive spillover” towards targeting autoimmune diseases. Biotech and pharmaceutical companies will be incentivised to further engineer these tools for autoimmune conditions specifically, a market that is expected to grow to 193$ billion by 2031 by IQVIA (from $154 in 2021). And given that autoimmune therapies have to pass higher safety thresholds than cancer ones, this is a good sign for age-related diseases: it means strategies that avoid side effects will be heavily pursued. As mentioned in the first section, we are already seeing this with Capstan, whose main selling point is avoiding lymphodepletion, precisely because this is too harsh of a side-effect for most autoimmune disease suffering patients (as opposed to those affected by cancer).
Although the first part of this essay was mainly focused on CAR-T therapies, it might be that for anti-aging immunosenescence targeting therapeutics, another modality is more suitable. These are bispecific T cell engagers (BiTEs): antibodies that can bind two antigens at once and direct T cells to kill a desired cell type — so far these therapeutics have shown promise in autoimmune disease, though there is less data than for CAR-Ts. Overall, BiTEs have shown less
I believe that when we understand the subpopulations of pro-inflammatory immune cells that drive age-related diseases better, these tools will be repurposed yet again, in the same way we saw a repurposing from oncology to autoimmunity. At some point, we might even deplete certain immune cell population preventatively and not just as a treatment. For this, we would need incredibly precise and safe modalities: the safety requirements for preventative anti-aging medicine will be higher than for any type of disease.
Although the first part of this essay was mainly focused on CAR-T therapies, it might be that for anti-aging immunosenescence targeting therapeutics, another modality is more suitable. These are bispecific T cell engagers (BiTEs): antibodies that can bind two antigens at once and direct T cells to kill a desired cell type — so far these therapeutics have shown promise in autoimmune disease, though there is less data than for CAR-Ts. Overall, CAR-Ts have shown more striking results in B cell malignancies in terms of pure efficacy: for example, a meta-analysis of success rates in of third‑line therapies in relapsed/refractory multiple myeloma (MM) found pooled complete remission rates of 54% for CAR T‑cell therapies versus 35% for bispecific antibodies (P < 0.01). There are many reasons for why CAR-Ts might be more efficacious, but, briefly TCR complex activation is usually not sufficient for target killing. CAR T cells provide co-stimulatory signals that BiTEs do not.

However, they also have higher risk profiles and are harder and more expensive to manufacture than BiTEs. Given the increased importance of safety/convenience in anti-aging therapeutics compared to cancers, unless issues like lymphodepletion are solved for CAR-Ts, BiTEs might actually be more promising long term for depletion of aging related immune cell subsets. This is particularly true for 2nd and 3rd generation BiTEs. What do I mean by a 2nd or 3rd generation BiTE?
For example, one could engineer BiTEs that include domains which increase their efficacy. For example, checkpoint inhibitory T cell engagers (CiTEs) comprise a BiTE core with an added immunomodulatory protein, which serves to reverse cancer-cell immune-dampening strategies (by incorporation of an anti‑PD‑1 Fv), improving efficacy. Although this is relevant to cancer, the chemical strategy (a version of click-chemistry) used to generate these CiTEs is what’s important here. One could imagine that for aging applications, one could use similar chemical methods to attach another molecule that improves efficacy (e.g. a cytokine like IL-2).
Besides this, modified BiTEs have another advantage for the future: we are getting better and better at AI modelling of antibodies, which means more complex BiTEs could benefit from that (although this discussion would warrant an entire new post).

affecting multiple organs.
blood malignancies are basically cancers of the immune system.
pretty much a “cure”.
this is an antigen expressed on most B cells.
e.g. imagine a CAR-T cell therapy that only targets cells that express CD19 *and* antigen X but do not express antigen Y.
this means that even if we can target a specific disease causing subpopulation with high precision, static information like scRNAseq might not be enough to tell us *which* subpopulation causes the disease phenotype and hence merits targeting.
cytokines are some of the molecules that CAR-Ts release which help destroy pathogenic cells.
For the biology nerds out there, the “secret sauce” of Capstan is that they make LNPs (the vehicles that carry the mRNA) cell type specific. In this case, T cell specific. In this case, they do so by attaching a CD8 antibody to the LNP, such that the mRNA is delivered only to CD8 expressing cells (so CD8+ T cells)

Their latest data in non human primates (NHPs) is in diseases like SLE, Sjogren’s and myositis.
who presumably had access to some internal data that I do not.
An autoantibody is an immune system protein that mistakenly targets and attacks the body’s own tissues instead of harmful invaders. They are associated with autoimmune conditions.
antigens are the proteins that exist usually on the surface of cells and trigger an immune response.
IgG is a type of antibody, which is a protein your immune system makes to help fight off infections.
CD8 T cell populations are immune cells that kill infected or cancerous cells by recognizing specific antigens, whereas B cells produce antibodies to target pathogens and mark them for destruction.
A coronary plaque is a buildup of fatty deposits, cholesterol, and other substances in the walls of the coronary arteries, which can restrict blood flow to the heart. Coronary plaque is a key feature of atherosclerosis, which is a condition where plaques build up in the artery walls, leading to narrowed or hardened arteries and reduced blood flow.
It may be true that we will see such spill overs but I’m not so sure this makes sense from an economic perspective. Autoimmune therapies are one of the few areas more attractive for Pharma than oncology. Consider the case of adalimumab (Humira), largest revenue drug in the world for several years. Anti-aging would be one of the few indications that would be even more lucrative than that! So you would expect spill overs to tend to be in the other direction. Does this just reflect the skew in basic research funding? Assuming all that research in mice is worth anything…
Do you have any theories on why it is that women are more prone to autoimmune disorders? Given pregnancy, it seems like there should be an evolutionary drive towards being less aggressive when confronted with something on the border of self and foreign, rather than more.