
IVF is not failing most women, oocyte ageing is
In which I point out why it all boils down to oocyte ageing and highlight some exciting new research into how this process happens

I saw the tweet below yesterday. The claim that “IVF (In vitro Fertilisation) is failing most women” jumped at me. "This can’t be right”, I said to myself. “Success rates of IVF for women below 35 are generally above 65% after 3 cycles!”

I went on to read the article, which was as bad as the title. This is rather unfortunate, because I fundamentally agree with the main message of the Economist piece: that we know little about female reproductive health & that we should invest more into understanding it! Indeed, I have written an entire piece about this ~ 1 month ago.
So how does this article arrive at the conclusion that IVF “fails most women”? There is little in the way of stats or evidence in the article, so it’s hard to say. The closest I could come to quantitative evidence is in this paragraph below:
“All too often, the pain and the cost come to nothing. The 770,000 IVF babies born in 2018 required some 3m cycles. Many women go through round after round of hormone injections, sometimes moving from one clinic to the next. In America and Britain roughly half go home with a baby in their arms, even after several years and as many as eight cycles of treatment.”
Firstly, I’d like to point out that, if “roughly half of women who undergo IVF walk with a baby in their arms”, it’s not really correct to say that “IVF fails most women”. But ~50% success rates still seems pretty low. The trick here is that they do not break this down by age. And given that women seeking IVF are more likely to be on the older side of the spectrum, this will bias results. Of course, the picture looks very different if you break the success rates by age (see below):

For women below 35, the success rate of IVF after 3 cycles is almost 70% (and can go up to 80-90% after 8 cycles). But there is a steep decline after that, getting to below 10% after 43!
By aggregating these ages together in their final calculation of success rates, the authors of the article are missing the crucial point that most of the cases where IVF are fundamentally due to female reproductive ageing, and not due to the process of IVF itself.
Why does this matter? Well, because I care about accuracy. But also, more pragmatically, it’s important that people know what is causing the issue of low success rates, so we can actually do something about it.
IVF used to have a success rate of only 6% per cycle when it was first introduced; This has increased to nearly 50% for women under 35 today. This is an undoubtedly dramatic improvement. A large proportion of this change is due to improvements in the culture media used for the embryos and the development of controlled ovarian stimulation, which allows multiple eggs to be retrieved per cycle. There is continued interest in improving the culture conditions of IVF to further increase efficiency, but this will only lead to marginal improvements unless we tackle what’s really important and driving overall success rates down: female reproductive ageing. And more specifically, as I show below, oocyte ageing.
It’s all about oocytes
Did you know that the oldest woman to give birth did so when she was 73? Yeah, you read this correctly, a woman gave birth at the age of 73! The doctors gave her a cocktail of hormones that helped her regain some reproductive ability and she carried a baby to term. There is a catch though: because the pregnancy was not using her own oocytes (or eggs1), her kids are not genetically related to her. She underwent post-menopausal IVF with donor eggs. For women who want biologically related kids, such a method is not available at such an advanced age. Pregnancies using own eggs are exceedingly rare after the age of 50, with the success of IVF at this age being incredibly low.
What this points to is that female reproductive ageing is mostly a matter of oocyte ageing.
This is reflected in charts of IVF success rates in women using own eggs vs donor eggs. The data reveals that as women age, if they use their own eggs, their odds of successful childbirth decrease rapidly. Yet, with eggs from younger donors, the decline is much more gradual. The divergence in success rates between using one's eggs versus donor eggs becomes apparent around 36 years of age. Notably, women over 40 using donor eggs have success rates comparable to those in their 30s, emphasising that IVF itself works just fine!

Why do oocytes age?
Unlike men, who produce new sperm continuously, women are born with a fixed number of occytes. Interestingly, this means the egg that developed into you once resided inside your grandmother!
But why do eggs deteriorate with age? What are the underlying biological reasons for this? We know way less than we should about this process, but it seems a large part of it has to do with DNA damage2.
And there is a particular type of DNA damage that oocytes are prone to, which is responsible for much of the decline in fertility with age: something called "aneuploidy". Aneuploidy means that the egg doesn't have the normal number of chromosomes. When there's either too many or too few, it can cause problems like infertility or miscarriage. As women age, the chances of their eggs having this chromosome issue increase significantly. Over half of the eggs in women > 35 can be affected. Now, why does this happen? It all boils down to a process called "meiosis."
Meiosis is how eggs (and sperm) are made, and its job is to ensure eggs get half the chromosomes of a regular cell; This means that when a sperm fertilises the egg, the embryo will have the correct, full complement of chromosomes: half from the mom and half from the dad. Meiosis is a complex process that encompasses several stages. Oocytes are arrested in the Prophase stage of meiosis while the future woman is still in utero! Meiosis resumes with ovulation, decades later, and leads to the formation of mature eggs that can be fertilised. So, for decades, oocytes exist in a “dormant” state, ready to be “awakened” by hormonal stimulation.

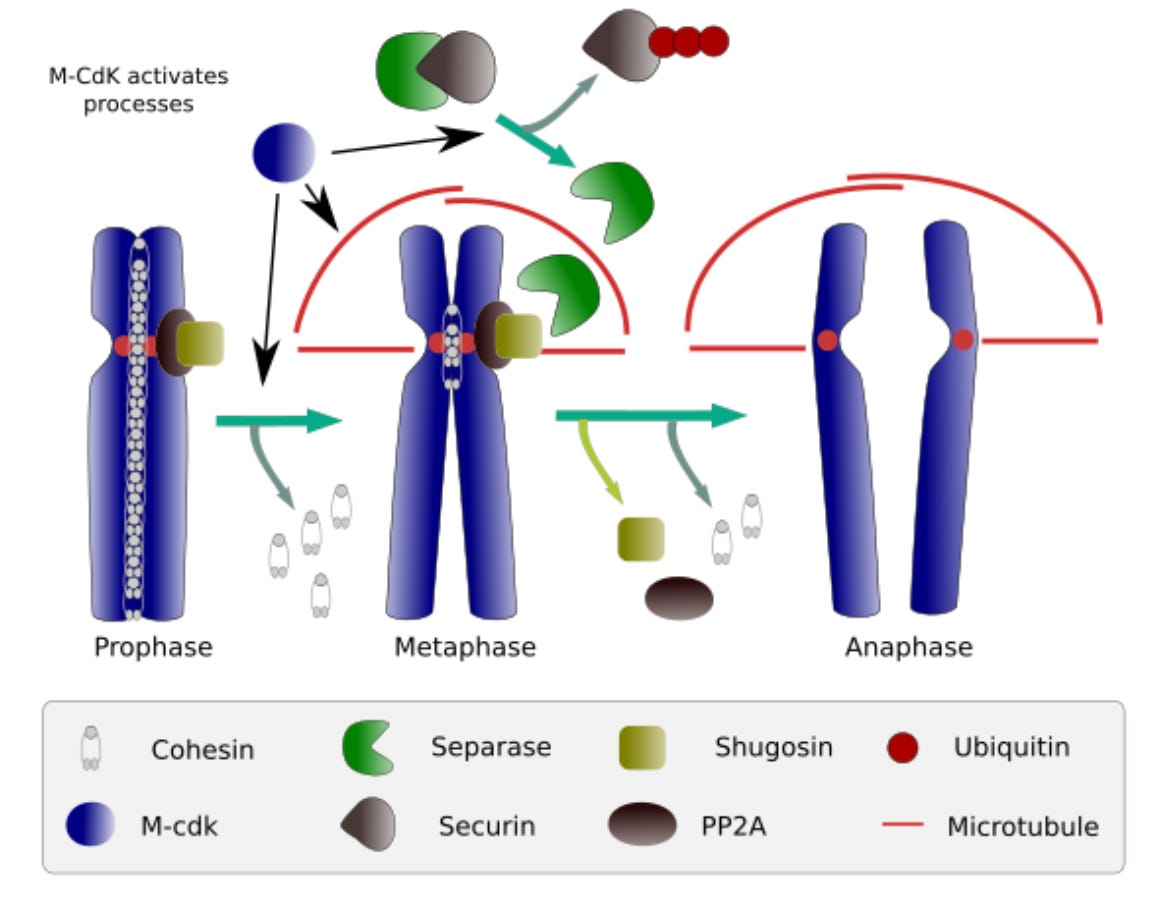
Of course, it’s crucial that while oocytes stay in this dormant state, they protect their genomic material. This is in large part done with the aid of a protein called cohesin. As you can see below, in prophase, cohesin acts like a glue, holding chromosomes together so that they separate correctly later on. The amazing thing is, this "glue" is set in place when a female is still in the womb and has to last her entire reproductive life. With age, this "glue" or cohesin seems to weaken, leading to errors in chromosome separation and thus affecting the egg's health and potential to lead to a successful pregnancy.
It's astonishing to realize that much of what I've discussed has only come to light in the past decade! This area remains somewhat uncharted, especially when you contrast our understanding here with fields like cancer. Just think: the groundbreaking paper revealing that age-related aneuploidy stems from a decline in chromosomal cohesion was published a mere 11 years ago.
There’s quite exciting research in this area, with researchers further gaining insight into what causes this loss of cohesion with age. Unfortunately, we are still in the early days of understanding oocyte ageing. I’ve written more about what are the current approaches to actually increasing female reproductive span in an earlier piece.
An oocyte is the immature female reproductive cell or germ cell, which, upon maturation, becomes an ovum or "egg". In human reproduction, the term "egg" often refers to the mature oocyte, which is released during ovulation and is capable of being fertilized by a sperm cell. I will use the terms interchangeably for the purpose of this essay, but they are not exactly the same!
DNA damage refers to changes in the structure of the genetic material within a cell that can disrupt its function and integrity. Protecting the oocyte from DNA damage is crucial because any genetic alterations can be passed on to the offspring, potentially leading to developmental abnormalities, diseases, or compromised reproductive potential.